
ABSTRACT
Syncope is a common complaint in clinical medical care. Except of neurological disorder, most of the patients havea brief benign clinical course with spontaneous recovery. Etiology may range from benign disorders to severe life-threatening diseases.Syncope as the leading symptom in patients suffering from intrathoracic neoplasm is uncommon. A rare case of a giant pleural solitary fibrous tumor causing recurrent episodes of syncope is presented. Diagnostic considerations and therapeutic strategy are discussed.
INTRODUCTION
Syncope is a common complaint in clinical medical care. It is defined as the transient loss of blood flow to the brain, secondary to hypotension after excessive vasopressor reflex. Drop in blood pressure caused by bradycardia or asystole results in transient conscious loss. In most cases syncope lasts for seconds to minutes with spontaneous recovery, characterized by benign clinical course. Etiology includes a variety of disorders and although an extensive evaluation is always undertaken, it is difficult to identify its cause. A case of a solitary fibrous pleural tumor associated with recurrent episodes of syncope is presented.
CASE PRESENTATION
A 45 year-old male was admitted to our Department complaining for sudden conscious loss lasting 2-3 minutes with spontaneous recovery during last month. All the episodes occurred while being on ordinary activity. The patient experienced visual field darkness followed by cold sweat, vertigo and finally syncope. Findings on physical examination of heart, lungs, abdomen and neurological system were normal. His medical record was clear without referring chest pain, shortness of breath, or palpitation before the episodes. Blood glucose, electrolytes as well as the rest blood chemistry results were found within normal bounds. A carotid sinus test assessed by carotid massage did not produce syncope or presyncope.
Non-specific findings on electrocardiography study were recorded. However, transthoracic echocardiography revealed compression of the left cardiac chambers by an intrathoracic mass without intracardiac thrombus, emboli or pericardial effusion. Chest x-ray showed a large lesion occupying almost completely the left pleural cavity (Figure 1). Chest Computed Tomography (CT) scans brought to light a giant tumor of the left hemithorax compressing both the left lung and heart without discrete mediastinal lymphadenopathy (Figure 2). The rest staging imaging studies [abdomen CT scans, brain Magnetic Resonance Imaging (MRI) and bone scan were negative for possible metastatic disease.

Figure 1. Chest x-ray depicting a large lesion occupying the left hemithorax.
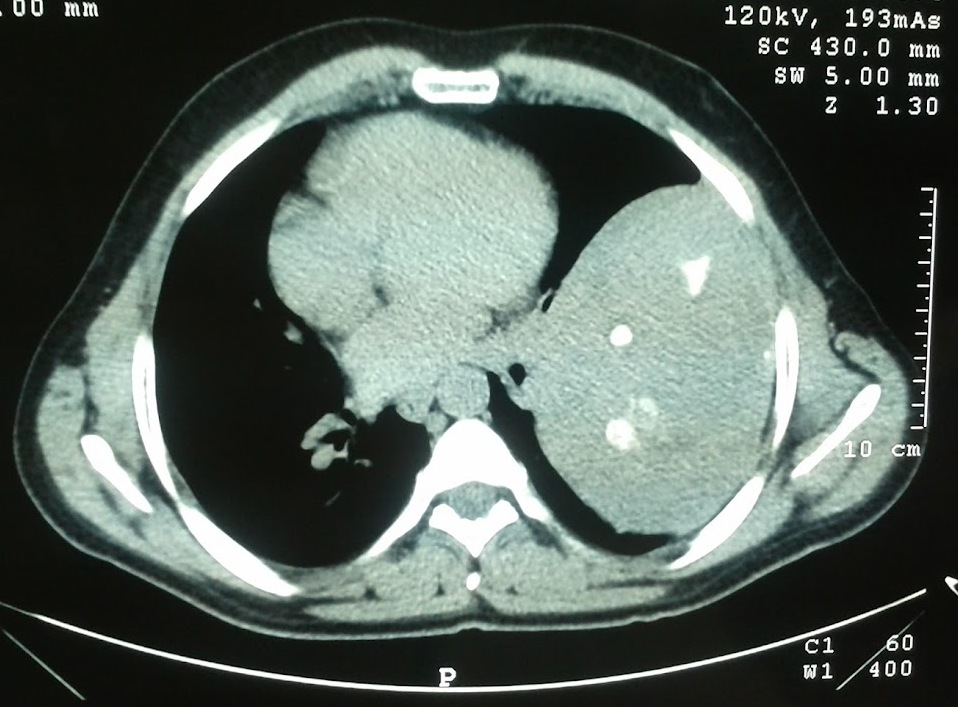
Figure 2. Chest Computed Tomography revealing a giant intrathoracic mass in the left pleural cavity. Compression of the left lung and heart is clearly indicated.
The patient underwent a left posterolateral thoracotomy and complete excision of the tumor was achieved. Intraoperative findings were consistent with a large tumor originating from the parietal pleura and attaching with an adhesion to the visceral pleura of the left upper lobe. The tumor was encapsulated without invading the lung, heart or great vessels and removed easily. Pathological diagnosis of a solitary pleural fibrous tumor with benign characteristics was reached (Figure 3).

Figure 3. Pathologic specimen. Tumor’s dimensions: 24x15x11cm.
Postoperative period was uneventful. Close one-year follow-up was negative for recurrence of syncope.
DISCUSSION
Syncope as the initial symptom regarding patients with intrathoracic neoplasm is rare. In most published cases, it is associated with the presence of mediastinal tumors. The cause of syncope is related to pulmonary arteries or cardiac involvement. Pulmonary embolism, cardiac arrhythmia or pulmonary artery hypertension appear as the possible mechanisms1.
A reduction of cardiac output by decreased venous return could also induce syncope2. Glossopharyngeal syncope associated with tumor of the oropharynx or base of the skull has been demonstrated3. Neurally mediated syncope can be directly induced by an intrathoracic lesion stimulating the vagus or phrenic nerve4,5. Neurocardiogenic syncope is characterized by syncopal episodes that are typically related to orthostatism. The underlying mechanism may be suggested by the clinical history, but recently the mechanism has been found to be reliably documentable with the head-up tilt test4. Syncope usually is caused by a primary drop in blood pressure, by bradyarrhythmias or asystole, or by a combination of these complications. Resumption of the supine position typically resolves the syncope and restores normal hemo-dynamic parameters.
Stimulation leading to syncope due to malignancy can be either mechanical or chemical6. The majority of these syndromes are secondary to constitutional factors related to baseline hypotension, vagal hyperactivity, or, most frequently, an excessive vasodepressor reflex, originating in the emptying but hypercontractile left ventricle. Most cases can be improved symptomatically by pharmacologic means (metoprolol, disopyramide, mineral corticoids), atrioventricular pacing, or both4,6. Para-neoplastic syndromes are infrequent and can involve any part of the nervous system, being degenerative, demyelinative, inflammatory, or necrotizing in nature7. They are associated with certain malignant neoplasms, specifically small cell carcinomas of the lung7. Usually neurologic symptoms precede tumor diagnosis by about 4 months. Autonomic dysfunction occurs in 10% of patients with paraneoplastic encephalomyelitis and sensory neuropathy8.In our case possible pathophysiological mechanisms include both compression phenomena and decreased venous return, as well as stimulation of the left vagus nerve.
REFERENCES
- Kpodonu J, Cusimano RJ, Johnston MR. An unusual cause of syncope. Asian Cardiovasc Thorac Ann 2005;13:400.
- Dubrava J, Drgona L, Kadlecik R. An unusual cause of recurrent syncope: Mediastinal lymphoma diagnosed with transesophageal echocardiography. Eur J Intern Med 2005;16 :204–6.
- Wallin BG, Westerberg CE, Sundlof G. Syncope induced by glossopharyngeal neuralgia: sympathetic outflow to muscle. Neurology 1984;34:522–4.
- Koga T, Kaseda S, Miyazaki N, et al. Neurally mediated syncope induced by lung cancer – a case report. Angiology 2000;51:263–7.
- Santambrogio L, Nosotti M, Palleschi A, et al. Solitary fibrous tumor of the pleura presenting with syncope episodes when coughing. World J of Surgical Oncology 2008;6:86-90.
- Angelini P, Holoye PY. Neurocardiogenic syncope and Prinzmetal’s angina associated with bronchogenic carcinoma. Chest 1997;111:819-22.
- Siemsen JK, Meister L. Bronchogenic carcinoma associated with severe orthostatic hypotension. Ann Intern Med 1963;58: 669-73.
- Dalmau J, Graus F, Rosenblum MK, Posner JB. Anti-Hu-associated paraneoplastic encephalomyelitis/ /sensory neuronopathy: a clinical study of 71 patients. Medicine 1992;71:59-72.
Author Disclosures: Authors Rallis Th, Asteriou Ch, Lazopoulos A, GogakosAS, PaliourasD, Chatzinikolaou F, Barbetakis N have no conflicts of interest or financial ties to disclose.
Corresponding author:
Christos Asteriou,
Al. Symeonidi 2, 54007,
Thessaloniki, Greece.
tel: +302310898314,
fax: +302310845514






