
Authors: Fyntanidou B1 MD, PhD, Veroniki F2 MD, PhD, Kolettas A3 MD, PhD, Ourailoglou V1 MD, PhD, Kotzampassi K4 MD, PhD, Theodosiadis P5 MD, PhD, Oloktsidou E1 MD, Karakoulas K1 MD, PhD , Grosomanidis V1 MD, PhD.
1Clinic of Anesthesiology and Intensive Care, School of Medicine, Aristotle University of Thessaloniki, AHEPA Hospital, Thessaloniki, Greece.
2Anesthesiology Department, “O Agios Dimitrios” General Hospital,Thessaloniki, Greece.
3Anesthesiology Department, “Saint Luke” Private Clinic, Thessaloniki, Greece.
4Department of Surgery, Aristotle University of Thessaloniki, AHEPA Hospital, Thessaloniki, Greece.
5Anesthesiology Department, Interbalkan Medical Center (Private Hospital) Thessaloniki, Greece.
Abstract
The interaction between increased Intra Abdominal Pressure (IAP) and Intrathoracic Pressure under different Positive End Expiratory Pressure (PEEP) levels is intriguing, since these two conditions coexist frequently in several clinical settings. The aim of our study was to investigate the interaction between different PEEP levels and increased IAP during laparoscopic cholecystectomy. In fifty two patients, who underwent scheduled laparoscopic cholecystectomy, cardiovascular parameters were determined by an Oesophageal Doppler Monitor device during two different time periods, before and after pneumoperitoneum, and under five conditions: (i) PEEP 0 cmH2O (ii) PEEP 5cm H2O (iii) PEEP 10cm H2O (iv) PEEP 15cm H2O and (v) in the absence of PEEP or ventilation. Cardiac output and stroke volume showed a statistically significant decrease compared to the baseline value after the application of different PEEP levels, when there was no pneumoperitoneum (p<0.05). However, both parameters increased, when PEEP and pneumoperitoneum were applied together (p<0.001). Corrected flow time, peak flow velocity in the descending thoracic aorta and mean acceleration showed similar alterations but not at all PEEP levels. Finally, αt the no PEEP or ventilation phase, the negative effects of increased IAP on the cardiocirculatory function were predominant. According to these results, application of PEEP seems to counterbalance the negative hemodynamic effects of increased IAP. Moreover, it could also be concluded that ‘ideal’ PEEP level might be the one that borders the IAP level, since the best cardiac output and stroke volume values were reported at that point.
INTRODUCTION
Application of Intermittent positive pressure ventilation (IPPV) induces cyclic changes in left and right ventricle loading. Transpulmonary pressure increase during inspiration induces a decrease in the preload and an increase in the afterload of the right ventricle (RV).1 This combination results in a reduction of RV stroke volume (SV) and cardiac output (CO).2-6 Notably, CO decrease is directly associated with airway pressure elevation and the resultant proportional intrathoracic pressure (ITP) increase.7,8
General anesthesia and mechanical ventilation (MV) can evoke intraoperative hypoxemia, even in patients with healthy lungs. The main causative pathophysiological mechanisms are airway collapse and subsequent occurrence of atelectasis. Moreover, cyclic closing and opening of the alveoli and small bronchi during MV is strongly associated with ventilator induced lung injury.9-13
Application of positive end expiratory pressure (PEEP) is generally recommended as a routine anesthesia practice, in order to prevent atelectasis and hypoxemia. Furthermore, PEEP has been widely applied both intraoperatively and in the Intensive Care Unit (ICU) setting in several cases, such as in patients with acute lung injury (ALI) or acute respiratory distress syndrome (ARDS), in obese patients, during one lung ventilation in thoracic surgery and after cardiac surgery.14-18
Despite the undoubted beneficial effects of PEEP on respiratory mechanics, its impact on cardiac function is complex and often unpredictable. According to the results of several studies, application of PEEP is associated with a negative influence on CO.19-23 The PEEP-induced increase in ITP leads to a restriction of venous return to the right ventricle, resulting in a fall in CO.7 In fact, this fall in CO is completely attributed to the decrease of left ventricle SV and the alteration of its determinants; heart rate is generally not affected by PEEP.24,25
Patients with increased intra-abdominal pressure (IAP) are part of the routine anesthesia practice, as the number of laparoscopic procedures performed has increased significantly over the past few years. In laparoscopic surgery, increased IAP is a result of carbon dioxide (CO2) insufflation into the peritoneal cavity. Moreover, increased IAP is seen in many other clinical conditions, such as in patients with intraabdominal pathology (trauma etc). Increased IAP is associated with respiratory, cardiovascular and central nervous system sequelae.28-31
Coexistence of increased IAP and PEEP is frequently encountered in many clinical conditions and is challenging, since their interaction and their combined hemodynamic effects remain unclear. The results of many studies in the literature are controversial. In some, the combination of PEEP and increased IAP seems to be detrimental for the cardiovascular system, whereas in others PEEP is considered beneficial due to its positive influence on respiratory mechanics without any negative hemodynamic effects.45,46
The aim of our study was to investigate the hemodynamic effects of different PEEP levels in a setting of increased IAP, namely in patients undergoing laparoscopic cholecystectomy.
MATERIAL AND METHODS
Fifty two patients scheduled for laparoscopic cholecystectomy were included in this study. All of the patients agreed to the study protocol by signing a written Informed Consent Form, which was approved by the Ethics Committee of our hospital. The exclusion criteria were oesophageal obstruction and recent upper gastrointestinal surgery or bleeding.
Before anesthesia induction, all patients received an initial Ringer’s Lactate bolus adapted to their body weight, in order to remedy the deficit due to preoperative fasting (approximately 1000ml), which was followed by an infusion of 2ml/kg/hr of crystalloids. After preoxygenation, anesthesia was induced similarly in all patients, via propofol 1.5-2mg/kg, fentanyl 4-6μg/kg and cis-atracurium 0.15mg/kg and maintained with sevoflurane and fentanyl.
After anesthesia induction and onset of MV, an arterial line and a Folley catheter were placed on each patient. Moreover, an Oesophageal Doppler Monitor device (ODM II) (G 974, Abbott Laboratories) was placed into the esophagus to determine the CO. ODM was advanced to a position of 30 to 35cm from the incisors in order to obtain the best waveform display on the monitor screen. The rest of the monitoring included ECG, invasive and non-invasive blood pressure measurement, capnography, BIS and respiratory parameters..
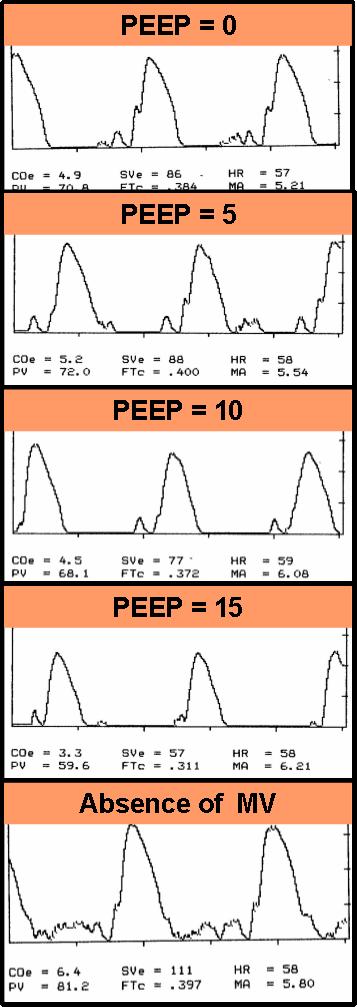 Figure 1. Period A: ODM Waveforms (traces) |
 Figure 2. Period B: ODM Waveforms (traces) |
For the statistical analysis the General Linear Model for repeated measures (ANOVA) was employed. Mean ± standard deviations are presented in the pertinent Tables. Statistical significance was set at p<0,05. PASW 18.0 (SPSS Inc., Chicago, IL) was used for data analysis. One-Sample Kolmogorov Smirnov test was applied at the beginning and for each individual parameter in order to find out whether data follow a normal distribution. In case data were normally distributed, Mauchly’s Sphericity was used to validate the correction method of the grades of freedom, which in all cases was the conservative Greenhouse-Geisser. The effects of pneumoperitoneum alone, of PEEP alone and of their combination on each parameter were examined. If the main effect of each separate factor was not significant, any parameter differences among the different study phases were ignored. If the main effect of each factor separately was significant, differences of the parameter along the different study phases were analyzed.
Results
Fifty two patients were enrolled in this study. Demographic data of the patients and their ASA-PS classification are presented in Table 1.
Table 1. Demographic data and ASA-PS classification
| P A R A M E T E R S | N | 52 |
| AGE (Years) | 49,5±14,4 |
|
| BODY WEIGHT (kg) | 77,8±18,4 |
|
| HEIGHT (cm) | 166±25,6 |
|
| BMI | 27,29±3,9 | |
| ASA-PS | I-III |
CO, SV, HR, FTc, MA, and PV alterations during A and B periods under the five protocol conditions are presented in Tables 2 and 3 respectively.
Table 2. CO, SV and HR alterations during the two study periods under five protocol conditions
| CO | SV | HR | ||||
| PERIOD | PERIOD | PERIOD | ||||
| A | B | A | B | A | B | |
| PEEP:0cmH2O | 4,7±1,7 | 4,2±1,5 | 72,1±23,4 | 65,2±18,2 | 66,4±9,4 | 65,1±18,2 |
| PEEP:5cmH2O | 4,6±1,6 | 4,6±1,4* | 70,2±23,7 | 69,2±18,5* | 66,2±9 | 69,2±18,5 |
| PEEP:10cmH2O | 4,1±1,6* | 4,9±1,5* | 64,3±22,4* | 72,3±18,5* | 64,7±9,1** | 72,3±18,5 |
| PEEP:15cmH2O | 3,6±1,7* | 4,7±1,5* | 57,7±22,7* | 73,5±19,9* | 64,7±8,8** | 73,5±19,9** |
| ABSENCE OF MV | 5,1±1,9* | 3,5±1,2* | 79,7±25,8* | 52,6±17,3* | 66±8,8 | 52,6±17,3 |
Table 3. PV, FTc and MA alterations during the two study periods under five protocol conditions
| CO | SV | HR | ||||
| PERIOD | PERIOD | PERIOD | ||||
| A | B | A | B | A | B | |
| PEEP:0cmH2O | 68,9±20,4 | 65,4±19 | 0,38±9,4 | 0,40±0,05 | 6,37±1,7 | 6,40±1,7 |
| PEEP:5cmH2O | 69,86±21,4 | 66,7±21,5 | 0,39±9 | 0,41±0,06 | 6,41±1,7 | 6,71±1,6 |
| PEEP:10cmH2O | 68,6±20,9 | 69,4±20,7* | 0,36±9,1* | 0,42±0,06** | 6,36±1,6 | 6,74±1,8 |
| PEEP:15cmH2O | 65,2±21,8* | 68,5±21,1** | 0,34±8,8* | 0,42±0,07 | 6,13±1,6** | 6,80±1,7** |
| ABSENCE OF MV | 71,3±20,8** | 59,5±19,8* | 0,40±8,8** | 0,38±0,6* | 6,58±1,7** | 6,23±1,7 |

Figure 3.Stroke volume alterations during the study period.

Figure 4. Cardiac output alterations during the study period
As far as HR is concerned, there was no statistically significant difference between the two study periods at any protocol phase. HR showed a statistically significant decrease at 10 and 15cmH2O PEEP during period A, whereas it showed a statistically significant increase at 15cmH2O PEEP during period B (Table 2).
FTc, which is considered as an indicator of cardiac preload47, showed a statistically significant decrease compared to the baseline value at 10 and 15cm H2O PEEP and a significant increase in the absence of MV during period A. During time period B, FTc showed a borderline statistically significant increase only at 10cmH2O PEEP and a statistically significant decrease in the absence of MV. The comparison of the two time periods revealed a statistically significant difference at all protocol phases (Table 3).
PV, which is an indicator of the left ventricular contractility,47 showed a statistically significant decrease at 15cm H2O PEEP and a significant increase in the absence of MV, compared with the baseline value, during study period. During time period B, PV showed a statistically significant increase at 10 and 15 cmH2O and a statistically significant decrease in the absence of MV. The comparison of the two time periods revealed a statistically significant difference only in the absence of MV (Table 3).
Finally, MA, which is a parameter mainly influenced by cardiac contractility and secondarily by after- and preload, showed a statistically significant decrease at 15cmH2O PEEP and an increase in the absence of MV during period A and an increase at 15cmH2O PEEP during period B. The comparison between the two periods A and B revealed a statistically significant difference only at 15cmH2O PEEP level (Table 3).
DISCUSSION
The negative impact of IPPV and PEEP on the cardiovascular system is well known and established in the literature.5,25,43,44
As far as the respiratory system is concerned, beneficial effects of PEEP application in the enhancement or preservation of oxygenation, the increase in FRC and the restoration of the ventilation perfusion disturbances are clear and beyond any doubt.12,13,15
However, the haemodynamic effects of high PEEP levels have been proven to be hazardous.7,19-21 This can be explained by PEEP induced preload decrease, afterload increase and alterations in the cardiac contractility.
Moreover, IAP elevation with or without MV has also negative effects on cardiovascular system.36-40 The magnitude of these effects is related to parameters such as the applied PEEP level, VT, IAP values and intravascular volume status. Hypovolemic patients are more susceptible to the adverse effects of increased ITP and IAP.
Since simultaneous presence of MV, PEEP and increased IAP is quite often in routine clinical practice both in the operating theatre and in the ICU, the interaction between IAP and ITP under different PEEP levels is of great importance.
Kraut et al studied the haemodynamic influence of the application of 10cm H2O PEEP in nine patients, who underwent laparoscopic cholecystectomy under 15mmHg IAP in anti-Trendeleburg position.45 They demonstrated preload and SV reduction in the presence of both PEEP and increased IAP, whereas the cardiovascular effects of increased IAP alone without any PEEP were well tolerated. They concluded that it would be advisable to avoid the combination of these two parameters in the daily routine clinical practice. Whenever this cannot be avoided, it is mandatory to monitor cardiac function and preload closely.
In our clinical trial, we evaluated the effect of different PEEP levels in a high intra – abdominal pressure setting during laparoscopic cholecystectomy. ODM was selected as capable of calculating real time SV and CO by measuring blood flow velocity in the descending aorta beat-by-beat.47,48 Besides SV and CO, other parameters such as PV, MA and FTc, which are correlated to ventricle contractility and preload, can be measured by this technique. ODM is a non invasive and more reliable method compared to the Swan-Ganz catheter thermodilution technique.50-52
In our study, we confirmed the negative influence of the incremental application of PEEP on CO and SV. Nevertheless, this influence was statistically significant only when PEEP exceeded 10cm H2O. Moreover, in the absence of both PEEP and MV, a great CO and SV increase was recorded. These results are consistent with previous studies in the literature.
After CO2 was insufflated and an intraperitoneal pressure of 12mmHg was obtained, CO and SV increased with the application of all three PEEP levels. Nevertheless, the most excessive increase in CO and SV was recorded with the application of PEEP of 10cm H2O and 15cmH2O, respectively, namely at the time when PEEP tends to counterbalance/equalize IAP. On the contrary, in the absence of both PEEP and MV, and while increased IAP was obtained, CO and SV showed a tremendous decline.
According to these results, PEEP application seems to counterbalance the negative haemodynamic effects of increased IAP. This can be derived from the statistical significant CO and SV increase compared to the basal measurement after the application of different levels of PEEP. Moreover, this correlation between PEEP and increased IAP may be more obvious by the detrimental CO and SV decline during time period B (pneumoperitoneum) and at the moment when both PEEP and MV are absent.
In addition to the above, we analyzed alterations of FTc as an index of cardiac preload.47,49,53 During period A, FTc showed a statistically significant decrease at 10 and 15cm H2O PEEP and a significant increase in the absence of MV compared to its baseline value, which are well reported effects of PEEP in previous studies. However, during pneumoperitoneum, FTc showed a gradual increase at all PEEP levels (statistically significant at 10cmH2O) and a statistically significant decrease in the absence of MV. This observation is very important since it implies that, during increased IAP, cardiac preload could be enhanced by PEEP application.
According to these results, we could also conclude that ‘ideal’ PEEP level may be the one that borders on the IAP level, since at that point we have reported the best CO and SV value.
A possible limitation of our study might be the use of ODM for CO measurements. ODM uses a normogram to estimate CO, which is based on flow measurements in the descending aorta and it seems that there is a good correlation between standard invasive methods such as thermodilution and ODM measurements.52-54 However, the fact that ODM calculates CO based on the assumption that 30% of the total blood flow goes to the upper body could cause errors in CO calculations in some situations with blood flow redistribution (such as aorta cross-clamping). Nevertheless, this was not the case in our clinical setting. Moreover, it is beyond any doubt that ODM provides a good guide of hemodynamic changes and clinicians should focus on trends rather than absolute values.
Our results have clinical implications, since increased IAP is a very common clinical condition not only in severely ill patients but also in patients undergoing any surgical laparoscopic procedure. In addition, MV with PEEP application is a standard ventilation strategy in general anesthesia. Indeed, PEEP application is often not just desirable but mandatory, because of ventilation/perfusion disturbances, especially in severely ill patients with intra-abdominal pathology of different causes. Therefore, specifically under these circumstances, the possible beneficial effect of PEEP not only on respiratory mechanics but also on the cardiovascular system seems very promising.
However, in situations when PEEP and increased IAP are applied at the same time, it is strongly recommended to closely monitor the heart function and to optimize preload, since both ITP and increased IAP have a negative effect on venous return.
Despite the positive results of this study and the possible favorable correlation of PEEP and increased IAP in relation to the cardiovascular system, more research and clinical studies are necessary to confirm this observation and to determine the ‘ideal’ PEEP level.
Conclusion
Our study showed that PEEP application at levels between 5cm H2O to 15cm H2O ,during MV of patients undergoing laparoscopic cholecystectomy, seems to protect the cardiovascular system from the negative hemodynamic effects of the increased intraabdominal pressure induced by pneumoperitoneum.
References
- Pinsky M. Recent advances in the clinical application of heart lung interactions. Curr Opin Crit Care 2002;8:26-31.
- Theres H, Binkau J, Laule M, et al. Phase related changes in right ventricular cardiac output under volume-controlled mechanical ventilation with positive end-expiratory pressure. Crit Care Med 1999;27: 953-58.
- Michard F, Teboul JL. Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation. Crit Care 2000;4:282-89.
- Duke Cardiovascular Effects of Mechanical Ventilation. Critical Care and Resuscitation 1999; 1: 388-99.
- Scharf S. Cardiovascular effects of positive pressure ventilation. Journal of Critical Care 1992 ; 7 : 268 – 79.
- Michard F. Changes in arterial pressure during mechanical ventilation. Anesthesiology 2005 ; 103 ; 419 -28.
- Cournand A, Motley HL, Werko L, Richards D. Physiological studies of the effects of intermittent positive pressure breathing on cardiac output in man. Am J Physiol 1948; 152: 162-174.
- Van den Berg P, Pinsky M. Systems approach to heart –lung interaction. The Netherlands Journal of Medicine 2000; 57 : 113 – 131.
- Hare GM, Kavanagh BP. Hypoxemia during surgery: learning from history, science, and current practice. Can J Anaesth. 2010; 57: 877-881.
- Müller J, Johannessen NW, Berg H, et al. Hypoxaemia during anesthesia-an observer study. Br J Anaesth 1991; 66(4): 437-444.
- Dreyfuss D, Saumon G. Ventilator-induced lung injury. Lessons from experimental studies. Am J Respir Crit Care Med 1998; 157: 294-330.
- Hedenstierna G, Edmark L. Mechanism of atelectasis in perioperative period. Best Practice and Research Clinical Anesthesiology 2010; 24 :157 – 69.
- Duggan M, Kavanagh B. Pulmonary atelectasis. A pathogenic perioperative entity. Anesthesiology 2005 ; 102 : 838 – 54.
- Hans G, Sottiaux TM, Lamy ML, et al. Ventilatory management during routine general anaesthesia. Eur J Anaesthesiol 2009; 26: 1-8.
- Veroniki F, Ourailoglou V, Fyntanidou B, et al. Intraoperative oxygenation impairment: A comparison between three alveolar recruitment strategies. The Greek E-Journal of Perioperative Medicine 2015; 13 : 41-57.
- Pelosi P, Gregoretti C. Perioperative management of obeses patients. Best Pract Res Clin Anaesthesiol. 2010;24:211-25.
- Grichnik KP, Shaw A. Update on one-lung ventilation: the use of continuous positive airway pressure ventilation and positive end-expiratory pressure ventilation–clinical application. Curr Opin Anaesthesiol. 2009; 22: 23-30.
- Dyhr T, Laursen N, Larsson A. Effects of lung recruitment maneuver and positive end-expiratory pressure on lung volume, respiratory mechanics and alveolar gas mixing in patients ventilated after cardiac surgery. Acta Anaesthesiol Scand 2002; 46: 717-725.
- Braunwald E, Binion JT, Morgan WL, et al. Alterations in central blood volume and cardiac output by positive pressure breathing and counteracted by metaraminol (Aramine). Circ Respir 1957; 5: 670-675.
- Rankin J, Olsen CO, Arentzen CE, et al. The effects of airway pressure on cardiac function in intact dogs and man. Circulation 1982; 66: 108-120.
- Smith P, Tyson GS, HammonJW, et al. Cardiovascular effects of ventilation with positive expiratory airway Ann Surg 1982; 195: 121-130.
- Van Trigt P, Spray TL, Pasque MK, et al. The effect of PEEP on left ventricular diastolic dimensions and systolic performance following myocardial revascularization. Ann Thorac Surg 1982; 33: 585-592.
- Van Hool Ch, Carilli A, Haronik E. Hemodynamic effects of positive end expiratory pressure. Am J Med 1986 ; 81 : 307 – 10.
- Viquerat CE, Righetti A, Suter PM. Biventricular volumes and function in patients with adult respiratory distress syndrome ventilated with PEEP. Chest 1983; 83: 509-514.
- Pinsky M. The hemodynamic consequences of mechanical ventilation: an evolving story. Int Care Med 1997; 23: 493-503.
- Tittley J, Fremes SE, Weisel RD, et al. Hemodynamic and Myocardial Metabolic Consequences of PEEP. Chest 1985; 88: 496-502.
- Fessler H. Heart lung interaction : application in the critically ill. Eur Respir J 1997 ; 10 ; 226 – 37.
- Karakoulas K, Vasilakos D, Grosomanidis V et al. Effects of pneumoperitoneum and LPS – Induced endotoxemia on cerebral perfusion pressure in pigs. Journal of Neurosurgical Anesthesiology 2006 ; 3 : 194-98.
- Kotzampasi K, Grosomanidis B, Dadoukis D, et al. Retroperitoneal compartment pressure elevation impairs pancreatic tissue blood flow. Pancreas 2007; 35: 169-172.
- Karakoulas K, Grosomanidis V, Amaniti E, et al. The effect of intra-abdominal hypertension alone or combined intra-abdominal hypertension-endotoxemia in cerebral oxygenation in a porcine model. Hippokratia 2008; 12 : 225-229.
- Safran D, Orlando R III. Physiologic effects of pneumoperitoneum. Am J Surg 1994; 167: 281-286.
- Feinstein H, Ghouri A. Changes in pulmonary mechanics during laparoscopic cholecystectomy. Anesth Analg 1993; 16(Sup): 102.
- Makinen M. Dynamic lung compliance during laparoscopic cholecystectomy. Anesth Analg 1994; 78: 261-270.
- Monk T, Weldon BC, Lemon D. Alterations in pulmonary function during laparoscopic surgery. Anesth Analg 1993; 76(Sup): 274
- Henderson W, Sheel W. Pulmonary mechanics during mechanical ventilation. Respiratory Physiology and Neurobiology 2012; 180 ; 162 -72.
- Kashtan J, Green J, Parsons E, et al. Hemodynamic effects of increased abdominal pressure. J Surg Res 1981; 30: 249-255.
- Ho H, Saunders C, Gunther R, et al. Effector of hemodynamics during laparoscopy: CO2 absorption or intra-abdominal pressure? J Surg Res 1995; 59: 497-503.
- Di Centa I, Coggia M, Cerceau P, et al. Total laparoscopic aortobifemoral bypass: short- and middle-term results. Ann Vasc Surg 2008; 22: 227-232
- Odeberg S, Ljungqvist O, Svenberg T et al. Haemodynamic effects of pneumoperitoneum and the influence of posture during anaesthesia for laparoscopic surgery. Acta Anaesthesiol Scand 1994; 38: 276-283.
- Kelman G, Swapp GH, Smith I, et al. Cardiac output and arterial blood-gas tension during laparoscopy. Br J Anaesth 1972; 44: 1155-1162.
- Motew M, Ivankovich AD, Bieniarz J, et al. Cardiovascular effects and acid-base blood gas changes during laparoscopy. Am J Obstet Gynecol 1973; 115: 1001-1012.
- Steingrub J, Tidswell M, Higgins T. Hemodynamic consequences of heart-lung interactions. J Intensive Care Med. 2003;18:92-99.
- Pinsky M. Heart lung interactions during mechanical ventilation. Curr Opin Crit Care 2012, 18:256–260.
- Pinsky M. Heart–lung interactions. Current Opinion in Critical Care 2007, 13:528–531.
- Kraut E, Anderson JT, Safwat A, et al. Impairment of cardiac performance by laparoscopy in patients receiving positive end-expiratory pressure. Arch Surg 1999; 134: 76-80.
- Meininger D, Byhahn C, Mierdl S, et al. Positive end-expiratory pressure improves arterial oxygenation during prolonged pneumoperitoneum. Acta Anaesthesiol Scand 2005; 49: 778-783.
- Singer M, Clarke J, Bennett ED. Continuous hemodynamic monitoring by esophageal Doppler. Crit Care Med 1989; 17: 447–452.
- Venn R, Rhodes A, Bennett E. The esophageal Doppler, In Vincent L. Yearbook of intensive care and emergency medicine 1999, pp 483 – 93.
- Singer M. Esophageal Doppler monitoring of aortic blood flow: beat-by-beat cardiac output monitoring. Int Anesthesiol Clin 1993; 31: 99-125.
- Schmid E, Spahn D, Tornie M. Reliability of a New Generation Transesophageal Doppler Device for Cardiac Output Monitoring. Anesth Analg 1993;77:971-81
- Baillard C, Cohen Y, Fosse J, et al. Haemodynamic measurements (continuous cardiac output and systemic vascular resistance) in critically ill patients: Transoesophageal Doppler versus continuous thermodilution. Anaesth Intensive Care 1999 ; 27 : 33-7
- Madan A, UyBarreta VV, Aliabadi-Wahle S, et al. Esophageal Doppler ultrasound monitor versus pulmonary artery catheter in the hemodynamic management of critically ill surgical patients. J Trauma. 1999 ; 46 :607-11.
- Singer M. Esophageal Doppler monitoring. In: Pinksy MR, Payen D (editors): Functional hemodynamic monitoring. Berlin Heidelberg: Springer-Verlag; 2005, pp. 193-204.
- Wong DH, Watson T, Gordon I, et al. Comparison of changes in transit time ultrasound, esophageal Doppler, and thermodilution cardiac output after changes in preload, afterload, and contractility in pigs. Anesth Analg 1991; 72: 584-588.
Author Disclosures:
Authors Fyntanidou B., Veroniki F., Kolettas A., Ourailoglou V., Kotzampassi K., Theodosiadis P., Oloktsidou E., Karakoulas K., Grosomanidis V. have no conflicts of interest or financial ties to disclose.
Corresponding author:
Fyntanidou Barbara
Anesthesia and ICU Clinic AHEPA University Hospital, Thessaloniki, Greece
Kautatzoglou 14A, 54639, Thessaloniki
T: 0030 6977427336
E-mail:






