
Authors: Petsas Dimosthenis MD, Griffiths Richard MD, FRCA
ABSTRACT
Fractures of the proximal femur are of the most frequent, especially in elderly patients. The increased frequency of these fractures highlights the need for effective management of those patients and the impact of these fractures regarding the cost to the national health system. The effects of pain in elderly patients is extremely aggravating, frequently leading to mental (confusion, delirium) and physical (cardiovascular) deterioration and complications.
The pain management of these patients in the emergency department (ED) with intravenous administered analgesics might complicate the status of these patients. The use of non-steroidal anti-inflammatory drugs (NSAID’s) might increase the risk of gastric ulceration, gastric haemorrhage and coronary syndromes, while the use of IV opioids–especially in elderly-incorporates the risk of respiratory depression, delirium, hypotension and constipation. The pain management of these patients with the use of fascia iliaca block applied in ED, or even in a prehospital setting from doctors of various specialties, paramedics or nurses seems to gain acceptance because of its steep learning curve, the simple technique, the high success rate and the low rate of significant complications.
INTRODUCTION
Fractures of the proximal femur are of the most common in elderly patients1. A great proportion of emergency orthopaedic/trauma cases are elderly patients with hip fractures. There were 61508 cases registered in the National Hip Fracture Database (NHFD), which includes data from 186 hospitals in England, Wales and Northern Ireland, from 1st April 2012 to 31st March 20132.
The size of the problem stresses the importance of hip fractures management and the impact on population’s quality of life. The increased cost on the health system is another important parameter. The 30–day mortality rates is approximately 8.2% in the UK and 13% in Denmark2.These two countries seem to have the most organized system of registries in relation to hip fractures.
The anaesthetic technique was not initially part of this national audit in the UK. Since 2011 the anaesthetic technique is an integral part of this audit and that fact led to the development of the Nottingham Hip Fracture Score. A main problem in this score remains the great variability of anaesthetic techniques applied on patients with hip fractures and the main efforts are to minimize this variability by introducing protocols of treatment in each hospital. The purpose of the Nottingham Hip Fracture Score is to estimate the postoperative morbidity and mortality in this specific patient subtotal3.
EFFECT OF PAIN ON ELDERLY PATIENTS
It is well recognised that pain might be the cause of many undesirable effects on several physiological processes, especially in elderly patients who are usually characterized by limited physiological reserves. There are conflicting publications in relation to pain threshold in elderly patients. Up to date preclinical data suggests that there is probably a reduction of the pain threshold in elderly (probably due to an age related increased sensitivity of pain receptors)4.
Mental and cognitive deterioration and delirium in elderly patients with hip fractures (because of the pain and maybe some subclinical emboli), is afamiliar picture during the preoperative visit to these patients. This specific relation between pain and mental/cognitive deterioration has been described in related papers. Presence of delirium is associated with incresead morbidity, increased length of hospital stay, increased health care costand poorer functional outcome results5.
In geriatric patients, the effect of pain on the cardiovascular system may be detrimental (due to increased catecholamines release, leading to tachycardia and hypertension). It seems that pain also negatively affects the immune system and delaying the normal process of healing6. All the prementioned facts highlight the need for fast and effective treatment of pain in elderly patients with proximal femur fractures in the emergency department or even in a prehospital setting, if this is possible, reducing the deleterious effects of pain and facilitating the transportation of these patients within the hospital.
The traditional approach of pain treatment in this subgroup of patients with intravenous administration of NSAID’s and opioids are related to an increased impact of side effects (GI ulceration, GI hemorrhage, increased risk of acute coronary syndromes, kidney injury, respiratory depression, constipation, disorientation and delirium). In addition, we should always take into account the changes of pharmacodynamics and pharmacokinetics in elderly patients.Those changes perplex the management of pain in elderly since they are complex and sometimes conflicting changes, making the calculations of the appropriate dosages very difficult7.
The application of Fascia Iliaca Block (FIB) in the emergency department by doctors from various specialties (consultants and trainees) must be established as routine practice. The learning curve of this technique is steep and with careful determination of the anatomical landmarks the complications are very rare and usually clinically non significant.
In the UK, the application of this block from other specialties, beside anaesthetists (like orthopaedics and emergency medicine doctors) is a routine, while prehospital application of the technique is encouraged aiming to an early and effective control of pain and prevention of its deleterious effects8.
The AAGBI (Association of Anaesthetists of Great Britain and Ireland–organization involved in the publication of the majority of the national guidelines in the UK) and RA-UK (RegionalAnaesthesia-UK) recently published a statement which refers to the possibility of FIB application by non-physicians after appropriate training. In the specific publication, it is mentioned that FIB should be considered a local anaesthetic technique rather than regional anaesthesia.
Of course in the case of application of FIB by non physicians AAGBI and RA-UK stresses the need for continuing audit regarding the effectiveness of the method and the possible complications9. In a recent publication from the Netherlands there is encouraging evidence from the application of FIB in a prehospital level from trained nurses, with very high success rate and encouraging results10.
ANATOMY OF THE FASCIA ILIACA COMPARTMENT
The fascia iliaca extends from the lower thoracic vertebrae to the anterior surface of the thigh. It covers the psoas major and the iliac muscle.
The fascia iliaca forms the posterior wall of the femoral sheath (lacuna vasorum) which contains the femoral artery and vein and the femoral branch of the genitofemoral nerve. In the femoral area the fascia iliaca is covered by the fascia lata and distally they merge. The fascia iliaca compartment is a «potential» space, which is defined:
–Anteriorly: By the posterior surface of the fascia iliaca, that covers the iliac muscle, with an extension in the midline which covers surfaces of the psoas major muscle.
–Posteriorly: by the anterior surfaces of the iliac and psoas muscle.
–Midline: from the vertebral column and cranially lateral by the medial edge of iliac crest.
–Upper / midline: in continuation with the space between quadratuslumborum and his fascia11.
HISTORY
The technique of injecting local anaesthetic into the fascia iliaca compartment was first described in a paper published by Dalensin in 1989. The specific article was describing the application of this technique in pediatric patients, comparing this with the 3 in 1 block (described by Winnie). The Winnie approach is a more “targeted” technique aiming closer to the femoral vessels and demanding the use of a nerve stimulator, making it a more complicated and demanding technique with a less steep learning curve12.
INDICATIONS, CONTRAINDICATIONS AND PRECAUTIONS
The Fascia Iliaca Block (FIB) has specific indications. Both adult and pediatric patients with pain in the region of the hip or with fractures of the proximal femur may benefit from the analgesic effects of the specific technique. It has a great variety of applications. Specific indications for the fascia iliaca block can be seen in table 111.
Table 1. Indications for Fascia Iliaca Block application.
| - Perioperative analgesia for patients with fractured neck or shaft of the femur |
| - Adjuvant analgesia for hip surgery depending on the surgical approach |
| - Analgesia for above knee amputation |
| - Analgesia for plaster application in children with femoral fracture |
| - Analgesia for knee surgery (always combined with sciatic nerve block) |
| - Analgesia for lower leg tourniquet (if patient was awake during surgery) |
| - Prehospital for easier retrieval of patient with proximal femur fracture. |
It can be applied in the prehospital setting, in the ED, to reduce pain during intrahospital transfers of patients and preoperatively making it easier for the patient to tolerate the sitting or lateral decubitus position for spinal anaesthesia, as well as minimizing the tourniquet–related breakthrough pain. Informed consent from the patient should always be sought before the block application in the ED.
Absolute contraindications of the method are patient’s denial, allergy or anaphylactoid reaction to local anaesthetics and open fractures. All the rest are considered relative contraindications and in general are those related with contraindications to local anaesthetics. Anticoagulation increases the risk of bleeding and hematoma formation, but is not an absolute contraindication and clinical assessing decision must be made. The application of FIB with the use of anatomical landmarks should be avoided in patients who underwent femoral bypass surgery in the past because of the alteration of the relative anatomy in the region (change of vessels anatomical position in relation to nerve branches)13.
TECHNIQUE OF FASCIA ILIACA BLOCK – ANATOMICAL LANDMARKS
The FIB blocks the nerves that are located in this potential anatomical space. The nerves included in this space are the femoral nerve (L2-L4), the lateral femoral cutaneous nerve (L2-L3) and the obturator nerve (L2-L4).
Blocking of the obturator with this technique is unpredictable. Of course this is of minimal interest for the management in the proximal area of the femur if we remember that in the majority of cases, the obturator is responsible for the sensory innervation of the region medial to the knee.
The FIB can be performed both with anatomical landmarks and with the use of 2D ultrasound guidance. The anatomical landmarks technique is based on the sensation of 2 consequetive losses of resistance (2 pop technique). In this paper we will mention the anatomical landmark technique since we are focusing on the application of the FIB outside the theatre and even in the prehospital level. This is because of its wider acceptance; it has a steeper learning curve and smaller need for training by non-anaesthetists in comparison with the ultrasound approach.
The anatomical landmarks for the FIB are the anterior superior iliac spine (ASIS) and the pubic symphysis. A line connecting the ASIS with the pubic symphysis is drawn. We then mark the tertiles on this line. The needle insertion point is 1-2 cm caudally to the point of junction between the middle and lateral tertile (Figure 1).
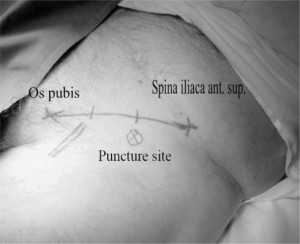
Figure 1. The anatomical landmarks of Fascia Iliaca Block. The line connects the anterior superior iliac spine (ASIS) and the pubic sym-physis. On this line the tertiles are marked. The needle point entry is 1-2 cm caudally on the junction between the middle and lateral tertile (‘x’ sign on the picture).The site of the femoral artery has also been marked.
A blunt needle (eg.Tuohy 18G) is introduced vertically to the skin until we feel two consequetive losses of resistance (the first loss of resistance is when we pierce the fascia lata and the second when we penetrate the fascia iliaca). Then we slowly aspirate to exclude intravascular placement of our needle and begin injecting the local anaesthetic. The administration of the local anaesthetic should be very easy on injection since we are injecting in an «empty» space. Any feeling of resistance on injection, implies wrong positioning of the needle and probably injection of the local anaesthetic inside muscle mass.
The volume of local anaesthetic injected should be at least 30 ml (with the possible exception of very frail and thin geriatric patients in which we should decrease the amount of local anaesthetic). The reason for that is because the FIB is a ‘compartment’ block, and not a block of a specific nerve so the compartment should be filled with local anaesthetic14. The fascia iliaca compartment can be seen as the yellow space in figure 2.

Figure 2. In this anatomical drawing the fascia iliaca compartment is highlighted with the yel-low colour. The first loss of resistance is felt when the fascia lata is punctured and the sec-ond loss of resistance when the fascia iliaca is penetrated. This drawing also shows the rela-tion to the femoral vessels and the site of injec-tion (red arrow).
In every nerve blocking technique there is a great variety of local anaesthetics, concentrations and volumes that can be used. The only restriction we should remember is that in the case of ‘compartment‘blocks we need a minimum volume of local anaesthetic able to fill this space. In our hospital, we use a volume of 30 ml Levobupivacaine 0.25%. After the local anaesthetic injection, the needle is withdrawn and pressure is applied distal to the site of the needle entry (in an effort to diffuse the anaesthetic centrally closer to the lumbar plexus, as described in Winnies 3 in 1 block).
The pain relief is usually fast. As a result the patient can more easily tolerate the changing position for a spinal anaesthetic.
The technique can be applied as a ‘single shot’ or a catheter technique. Of course we should never forget that the definite pain therapy for the proximal femur fractures is the surgical repair.
TROUBLESHOOTING
There are specific problems and difficulties that might be encountered during a FIB. The most frequent problems as well as the suggested appropriate action are seen in Table 2.
Table 2. Problems and troubleshooting with FIB
| Problem | Suggested action |
|---|---|
| - No distinct ‘pops’ are felt during needle advancement | Withdraw needle, check landmarks,change angle to more perpendicular or more cranially |
| - Hitting bone on needle advancement | Too deep, change angle redirecting more cranially |
| - Blood on aspiration | Remove needle, apply pressure for two minutes. Reattempt directing more laterally |
| - Resistance to injection of local anaesthetic | Slightly redraw needle, possible intramuscular positioning |
| - Pain on injection | Localised slight burning sensation around the site might be normal. Slow injection. Severe pain is not normal. Stop injecting |
| - Signs of local anaesthetic toxicity | Stop injection, call for help, give high flow oxygen, provide life support as required |
| - No pain relief within 30 minutes | Inject further 20 ml of low concentration local anaesthetic, consider alternatives for pain relief |
EFFECTIVENESS OF FIB – THE EVIDENCE
Pain assessment in geriatric patients might be a daunting and complicated task. The majority of elderly patients find it difficult to understand or to cooperate during the application of the frequently used pain scales (eg. VAS pain score, Verbal Rating Score, etg). This is a complicated problem involving both mental problems and physical disabilities. In this subgroup of patients a mental test should be an integral part of pain estimation.
A very practical approach to assess the mental state is a 9-point mental test, developed in Denmark (Hindsoe’s test). This test was developed because approximately 20 % of elderly patients were unable to participate in a Mini Mental State Examination (MMSE) interview. Each positive answer in this test gives 1 point. The Hindsoe mental test can be seen in Table 3.
Table 3. Hindsoe’s mental test.
| Can account for own age | Yes | No |
| Can account for own social number | Yes | No |
| Can account for home address | Yes | No |
| Can account for own phone number | Yes | No |
| Can account for own weight)+ 5% | Yes | No |
| Can account for date of hospitalization | Yes | No |
| Can account for own medication (type-not names) | Yes | No |
| Can identify the interviewer after 30 minutes | Yes | No |
| Total score (SUM): 0 1 2 3 4 5 6 7 8 9 | ||
A score less or equal to 6 (<6 ) is considered to represent cognitive impairment15.
Practically for the assessment of the efficacy of the FIB most geriatric anaesthetists uses the passive flexion of the hip. An increase in the pain–free flexion of the hip over 10, marks a significant reduction of pain.
The success rate of the FIB applied with the use of anatomical landmarks varies from 67% to 96% in various publications16,17.
This great variance in the success rate can easily be explained by methodology differences in the various publications (eg. the person who applies the FIB might be an anaesthestist, ED doctor, orthopaedics or paramedics).
COMPLICATIONS
Regarding the complications of the specific technique, there is a great variance in complication reports in the literature. The complications varies from 0% to approximately 10%. These reports include even minor symptoms as complications (such as redness, burning sensation etg). Complications related to local anaesthetic toxicity varies from 0-1%, but usually there are some early toxicity signs from CNS, who do not evolve to cardiovascular symptoms. The majority of complications are clinically not significant, such as redness, hematoma formation and bruising.
In a series of 187 patients who underwent a FIB applied with anatomical landmarks by junior registrars in Emergency Medicine, the only reported complications were 2 cases of mild CNS symptoms (possible due to bupivacaine toxicity)18-22. As it is well known, in cases of local anaesthetic toxicity, the symptoms from CNS (confusion, blurred vision, agitation, seizures) preceed the symptoms from the cardiovascular system (hypotension, bradycardia, arrhythmias). According to AAGBI, there is no need for prolonged monitoring with the specific technique. On the contrary, AAGBI stresses the importance of «screening questions» in relation to local anaesthetic toxicity symptoms.
In paediatric patients high plasma ropivacaine levels have been reported after FIB application without any clinical signs of local anaesthetic toxicity. This specific study had a very small study size (n=6 patients) and the investigators administered 3.5 mg /kg BW of ropivacaine23.
We should always remember that in classical books of regional anaesthesia it is mentioned that there is no strong correlation of local anaesthetic peak plasma concentration and clinical signs of toxicity24.
REFERENCES
- Cooper C, Campion G, Melton LJ. Hip fractures in the elderly: a worldwide projection. Osteoporosis Int 1992;2:285-289.
- The national Hip Fracture Database. http://www.nhfd.co.uk/
- Hogh A, Dremstrup L, Jensen SS, et al. Fascia iliaca compartment block performed by junior registrars as a supplement to preoperative analgesia for patients with hip fracture. Strat Traum Limb Recon 2008;3:65-70.
- Yezierski RP. The effects of age on pain sensitivity: pre-clinical studies. Pain Med 2012(suppl 2);13:27-36.
- Pompei P, Foreman M, Rudberg M, et al. Delirium in hospitalized older persons: outcomes and predictors. J Am Geriatr Soc 1994;42:809-815.
- Wells N, Pasero C, McCaffery M. Improving the quality of care through pain assessment and management. http://www.Ahrq.gov
- Kaye AD, Baluch A, Scott J. Pain management in elderly people: A Review. The Oschner Journal 2010; 10:179-187.
- Lopez S, Gros T, Bernard N, et al. Fascia iliaca compartment block for femoral bone fractures in prehospital care. Reg Anesth Pain Med. 2003 May-Jun;28(3):203-7.
- AAGBI POSITION STATEMENT 2013. Fascia Iliaca Blocks and Non-Physician Practitioners.
- Dochez E,Van Geffen G, Bruhn J, et al. Prehospital administered fascia iliaca compartment block by emergency medical service nurses, a feasibility study. Scand J Trauma Resusc Emerg Med 2014;22:38
- Range C, Egeler C. 2010. Fascia iliaca compartment block: Landmark and ultrasound approach. http://www.frca.co.uk
- Dalens B, et al. A comparison of the fascia iliaca block with 3 in 1 block in children. Anaesth Analg 1989;69:705-713.
- Bolch S. Fascia iliaca block, guidelines for use in the Emergency department.http://www.asem.org.au/
- Hanna L, Gulati A, Graham A. The role of fascia iliaca block in hip fractures: A prospective case control study and feasibility assessment of a junior doctor delivered service. ISRN Orthopedics 2014; article ID191306.
- Kristensen MT. Hip fractures, functional assessments and factors influencing in-hospital outcomes, a physiotherapeutic perspective. Thesis. Lund University, Sweden.
- Hwang U, Richardson LD, Sonya TO, et al. The effect of emergency department crowding on the management of pain in older adults with hip fracture. J Am GeriatrSoc.2006;54:270-275.
- Foss NB, Kristensen BB, Bundgaard M, et al. Fascia iliaca compartment blockade for acute pain control in hip fracture patients:a randomized placebo controlled trial. Anaesthesiol 2007;106:773-778.
- Godoy MD, Iserson KV, Vazquez JA. Single fascia iliaca compartment block for post hip fracture pain relief. J Emerg Med 2007;32(3):257-262.
- Hauritz RW, Gerlif C, Ronholm E. Fascia iliaca block performed by emergency medicine trainee physicians in hip fractures. Ugeskr Laeger 2009;171(7):515-518.
- Wathen JE, Gao D, Merritt G, et al. A randomized controlled trial comparison of fascia iliaca block to a traditional systemic analgesic for femur fractures in a pediatric ED . Ann Emerg Med 2007;50(2):162-171.
- Black KJ, Bavan CA, Murphy NG, et al. Nerve block for initial pain management of femoral fractures in children. Cochrane Database Syst Rev 2013 Dec17;12:CD009587.
- Monzon DG, Vazquez J, Jauregui JR, et al. Pain treatment in post traumatic hip fractures in the elderly: regional block vs systemic NSAID’s. Int J Emerg Med 2010;3:321-325.
- Paut O, Schreiber E, Lacroix F, et al. High plasma ropivacaine concentrations after fascia iliaca compartment block in children. Br Journal Anesth 2004; 92(3):416-418.
- MacLeod GA, Butterworth JF, Wildsmith JAW. Local anaesthetic systemic toxicity. In Cousins MJ, Carr DB, Horlocker TT, Bridenbaugh PO (Eds): Neural blockade, 4th edition, Lippincot Williams & Wilkins, 2009,pp.114-132.
Author Disclosures:
Authors Petsas D, Griffiths R have no conflicts of interest or financial ties to disclose.
Corresponding author:
Dimosthenis Petsas MD,Trust Registrar
Anaesthesia Department
Peterborough City Hospital,
Cambridgeshire, UK.
Tel: 00447530598212
E mail:






