
Authors: Changaei F1 PhD, Simbar M2 PhD, Irajpour A3 PhD, Akbari S4 MD
1Department of Nursing and Midwifery, Lorestan University of Medical Sciences, Khorramabad Iran
2Department of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Nursing and Midwifery Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
4Medical Department, Lorestan University of Medical Sciences, Khorramabad, Lorestan, Iran
ABSTRACT
Access to appropriate and high quality health care is one of the most important ways to reduce maternal and infant mortality. This study evaluates the quality of care during childbirth, the effective factors, and promoting strategies in Lorestan province, Iran. This research is a mixed explanatory study (i.e., quantitative and qualitative). The quantitative part is descriptive-analytic. The quality of 200 care processes during childbirth was assessed in the health centers of the province. The data were gathered through the checklists prepared according to the guidelines of the Iranian Ministry of Health. Statistical analysis was performed using SPSS software. In the qualitative part, the strategies for solving the problem were assessed through interviews with service providers, maternity administrators, and senior decision-making university officials. According to our results, the levels of care quality during childbirth were intermediate in all four phases. The lowest levels of quality in the first, second and third stages were associated with Leopold’s maneuver, hand washing and pulse control, respectively. Based on the interviews, the main reasons for the reduction of care quality include lack of staff’s motivation, overcrowding and shortage of nursing workforce, low attention of officials to the Department of Midwifery, and the high burden of writing in the maternity. To improve the quality of services, the authorities in Lorestan University of Medical Sciences propose strategies such as making some incentives for care promotion. Considering the quality of care during childbirth as intermediate in all four stages in the province and investigation of the reasons indicating the lack of sufficient incentive in midwives, it is recommended that strategies such as financial incentives, greater use of private sector to reduce public sector workload, quality increase and further use of in-service training to improve the quality of services be adopted.
Introduction
Maternal health improvement was set as one of the eight Millennium Development Goals (MDGs) of the World Health Organization (WHO) in the meeting held in 20001. Two important criteria to achieve this goal include reducing maternal mortality by three-quarters in 1990 and women’s access to reproductive health services by 20152. Maternal mortality is not only a health indicator, but also one of the indicators of a community’s development showing how much societies care about maternal health3. The most important cause of maternal death is pregnancy-related complications, being responsible for 18% of women’s diseases in developing countries4. The estimated maternal mortality rate in Iran was approximately 24.6 per hundred thousand live births in 20085. Based on mortality statistics, maternal mortality rate in Lorestan province was slightly higher than that of the country in 20106. Some strategies were proposed to reduce maternal mortality such as increasing women’s literacy, skilled attendance at delivery, family planning, pre-pregnancy and prenatal care as well as during- and after-childbirth (postpartum) care3. Approximately, more than one quarter (i.e., 300 million) of adult women in developing countries suffer from chronic diseases and injuries related to pregnancy and childbirth 7.
It is shown that in the case of supplying resources and availability of sufficient services, many of these deaths are preventable8. Maternal mortality rate can be significantly reduced if the labor is performed under the supervision of a skilled and educated staff. Appropriate midwifery care is also a vital factor in the reduction of maternal mortality9. Reducing maternal and child mortality rates has constantly been one of the main goals of the WHO activities. Prenatal care, as well as during- and after-childbirth care, is the key strategy to achieve this goal10. Despite the efforts of the WHO, UNICEF, the World Bank, and other organizations to reduce maternal mortality by three-quarters up to 2015, there is little progress and the situation is worsened in some areas8. To achieve optimum results during pregnancy and childbirth and after childbirth, some activities have been conducted by skilled and well-educated groups11. In Iran, 98% of deliveries are performed by trained staff , and the prenatal care coverage is more than 98%. Women and babies care during childbirth is the most common cause of hospitalization12.
The purpose of health care during childbirth is to achieve the highest level of mothers’ and babies’ health with minimal interventions13. In line with the global reproductive health goals and strategies at the International Conference on Population and Development held in the WHO, the Iranian Ministry of Health and Medical Education has assigned improving the quality of reproductive health care and family planning as one of its priorities12. Maternal mortality reduction is among the important goals of the foregoing Ministry from 30 in 1990 to 18 per one hundred thousand in 2015. Since the rate reduction of maternal mortality is slower than the anticipated program (reduced rate is 3.2% per year, which should be 5.5% per year)14, concerted efforts should be made to expedite the process of reducing mortality. Thus, one of the most important measures is to evaluate and improve care quality.
In a study entitled the quality of midwifery care provided for the women admitted in the selected maternity wards of the selected hospitals of Kordestan University of Medical Sciences, it is mentioned that the quality of care in the first and third stages of labor was optimum, but it seemed intermediate in the second stage of labor15. Based on the results from the analysis and comparison of the physical and psychosocial quality of care during labor, it was shown that the quality of care is undesirable and more attention is required on the part of the authorities and service providers16.
MATERIAL AND METHODS
The content validity index (CVI) method was used to evaluate the content validity. Therefore, a questionnaire was emailed for 15 faculty members, expert in the subject at Lorestan and Isfahan Universities of Medical Sciences. They were asked to allocate one of the four degrees of “irrelevant, low correlation, related, and closely related” to each question according to form and content. An alternative part was also considered to record their comments (content validity ratio or CVR=0.82)19. To determine the face validity of the questionnaire, during interviews with a limited number (including 15 participants) of the target population, if a question was unclear for the respondents, it was edited. The final modification was performed according to the experts’ comments. To assess the reliability of the observational checklist, intra-rater reliability assessment method was used, which was approved by the 0.86 score of the Pearson correlation coefficient.
Having received permission from Lorestan and Isfahan Universities of Medical Sciences, the interviewers referred to the public hospitals affiliated to these universities in the morning, afternoon and night shifts for sampling and completing the questionnaires. The data were gathered via checklists by observing the process of childbirth care at different stages of labor. Finally, the collected data were analyzed by SPSS software (ver.16).
In the second part (i.e., qualitative study with content analysis), according to the acquired scores, the issues that needed improving were determined and the interview questions were formulated. After conducting in-depth interviews or focus group discussions with the maternity staff, each lasting for 45-90 minutes, primary causes and strategies were investigated. Using conventional content analysis of the interviews, the questions related to the specialized strategies to enhance the quality of care20 were designed. Moreover, by conducting focus group discussions with 12 experts (or maternity officials), specialized strategies were examined. General strategies to improve the quality of care during and after delivery were also assessed through individual interviews with 21 officials and decision- makers in Lorestan University of Medical Sciences.
RESULTS
The quantitative part
In this study, 200 childbirth cares were assessed at each stage. The results showed that, in the first stage of labor care, satisfaction of delivery room cleaning was desirable in most fields, which gained more than 67% of the total score. Only in providing some labor cares such as Leopold’s maneuver (10.8%), pulse control (32.4%) and fetal heart rate control by Pinard (fetoscope) (3%), the scores were lower than 33% and the quality was poor. In the second stage of labor in most fields of labor care, the obtained score was desirable. However, only in some fields such as hand washing, heart rate monitoring, and heart rate control by Pinard, the score was lower than 33% of total score and the quality was poor. Notably, the lowest score related to heart rate control by Pinard. At this stage, blood pressure control and readiness for delivery gained 34-67% of the total score and had the moderate quality. Other cases had desirable quality. In the third stage of labor, only the score of pulse control was less than 33% of the total and care quality was poor. Blood pressure control and neonate examination had scores of 34-67% of the total and showed moderate quality. In other cases, care quality was desirable.
Generally, the quality of care during labor was average in all four stages in the province (Table 1). The results showed that, in some fields at different stages of labor, care quality was almost the same in most cities. Accordingly, it was observed that in most cities, some fields of the first stage of labor such as history taking, vaginal examination, fetal heart rate (FHR) control by Sonicaid and blood pressure control had good quality. In the second stage of labor, some fields such as fetal heart rate control by Sonicaid, physical care and emotional support, evaluation of labor process and blood pressure control showed optimum quality. In the third stage of labor, blood pressure control, physical care and emotional support, assessment of the episiotomy repair, placental removal evaluation as well as evaluation of immediate care of the newborn and evaluation of labor reports had good quality in most cities. In the fourth stage, the quality of bleeding control and breastfeeding training were desirable. Some cases such as the midwife’s relationship with the patient and Leopold’s maneuver had poor quality in the first stage of labor. In the second stage of labor, hand washing and, in the third stage, blood pressure control had poor quality in most cities. The quality of postpartum care in the first two hours of delivery had average quality with 65% of the total score at this stage.
Table 1. Quality of care during childbirth provided in the health centers of Lorestan province according to the delivery stages
Note: The numbers show percent of frequency.
Degree of care quality
Condition
Delivery stagesDesirable
68-100%Intermediate
34-67%Undesirable
0-33%Mean degree of quality
First 14 83 3 54.50%
Second 24.6 71.4 4 57%
Third 57.9 38.5 3.6 66%
Fourth 46.9 51.5 2.6 65%
The qualitative part
The analysis of hospital staff interviews showed that the major cause of reduced quality in certain fields of care includes inadequate trainings, weakness in professionalization, inadequate staff’s motivation, insufficient work force, inadequate staff’s motivation, high burden of writing in the hospital, and inattention of officials to midwives (Figure 1).

Figure 1. Effective factors on quality of care during childbirth (Source: Research results)
In the focus group, strategies of improving the quality of care were discussed. The results showed that maternity authorities consider some items for the improvement of quality such as recruiting more midwives to reduce the workload per shift, increasing financial incentives to encourage midwives to provide high quality services, more attention to midwifery, assignment of the bulk of the mothers’ training to staff working in health departments to have more effective trainings during pregnancy, midwifery on-call employment to reduce workload and increasing the quality in busy shifts, assignment of responsibilities of women’s specialty hospitals to more expert staff in the field of women (midwives) to facilitate specialized activities, increasing the quality and repeatability of in-service training and motivation of staff for greater embracing in these trainings.
At the end of the project, different approaches to improve care quality from the viewpoint of Lorestan University of Medical Sciences’ authorities were investigated. The results indicated that there is no consensus among the officials and the staff in some cases, including inattention of authorities to midwifery, staffing lack and lack of adequate incentive in midwives as the main causes of declining quality of care. In other words, the officials rejected the foregoing causes as quality-reducing factors. According to the evidence cited by the officials, the average staffing force in the provincial hospitals was within the standard limit. Inappropriate distribution of staff in different shifts and unpredictability of maternity patients are the causes of crowding or lack of work force. In addition, strategies such as strengthening the private sector to reduce public sector’s workload, increasing the staff’s motivation through encouragement and financial assistance are also suitable for providing high quality service. To improve the quality of in-service training and embracing the staff to attend in these classes, some strategies are recommended, which include counting the training hours as their shift work or overtime, counting the mission for people participating in the training course in the province center, and subjecting the annual granting to participate in these classes. Some of these measures are already extensively implemented. The authorities agreed on assigning the responsibilities of women’s specialty hospitals to more experienced expert staff in obstetrics and gynecology, and mentioned that, considering the availability of the context (i.e. suitable and competent applicant), they are willing to cooperate (Figure 2).
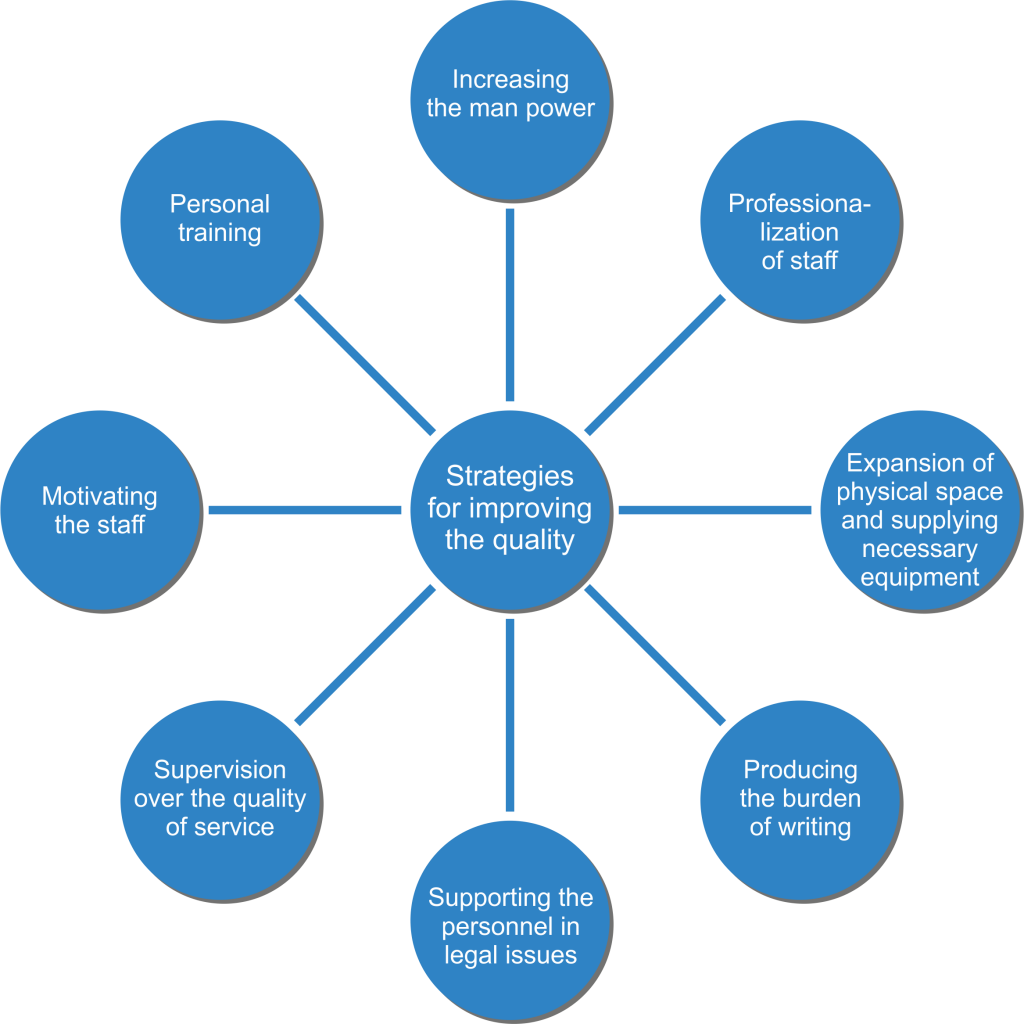
Figure 2. Improving strategies for quality of care during childbirth (Source: Research results)
DISCUSSION
The results suggested that the care quality offered in most fields of the first stage of labor in Lorestan province were moderate or desirable; only in a few cases including Leopold’s maneuver and controlling the pulse, it was poor. With a little contemplation on the results, it was shown that there is a high level of compliance (more than 90%) of fetal heart rate monitoring with Sonicaid in the first and second stages of labor in most cities, indicating the ease of use and availability of this tool. These features lead to the replacement of Pinard with Sonicaid. After listening to the heart rate with Sonicaid, assessment of the history had the highest compliance rate with the desirable conditions. Leopold’s maneuver is one of the easiest ways to identify fetal position and presentation; location of the fetus’ organs, the presence or lack of engagement and descent. In addition, the weight and size of the fetus can also be estimated by this method, all demonstrating the importance and usefulness of this measure during childbirth. Leopold’s maneuver can be easily handled with spending as little time as possible. We noticed the poor quality of this care in the health centers of the province; thus, the causes should be investigated. One probable reason is inadequate understanding of the importance of this care by the employees21. However, due to the standard ratio of midwifery staff during childbirth, one midwife for each caregiver in labor22, and the failure of this standard ratio in the medical centers of Lorestan, the lack of midwives leads to overwork pressure and insufficient efficacy of midwives in the maternity ward, finally causing less consideration to some cares, which can be ignored by other measures such as vaginal examination. One of the essential procedures during childbirth is monitoring vital signs such as pulse rate control of woman-in-labor in the first stage, which should be performed once in each four hours23. However, the results of this study indicate the poor quality of offering this care in the health centers of the province.
The use of paretograph is a measure currently used in the health care centers, which leads to the increase of quality and regularity of examinations of mother and fetus during childbirth and quick detection of any problems. This graph allows the midwife to indicate delivery details24. When electronic monitoring of fetus is not provided in the all health centers, partograghy can be effective for more accurate assessment of fetal and maternal health as well as managers’ better evaluation of service providers’ performance. In this study, the quality of partogram in the health centers of the province was average and should be promoted.
In the second stage of labor, the scores of some kinds of care such as hand washing and pulse control were less than 33% and had poor quality. Considering the importance of blood pressure control during childbirth, although the score was more than 33%, it has poor quality and there is a need for improvement. Hand washing is one of the five main factors of patients’ safety declared by the World Health Organization25 and hygiene, including hand washing, is the first and foremost need to manage the delivery. During different stages of childbirth, hygiene is more important than antibiotics for preventing infection26. Unfortunately, this measure was of poor quality in the treatment centers of the province; which is apparently due to less attention of service providers in the province. Thus, the training classes can be effective in these areas.
Physical care and emotional support are among the high quality childbirth care in all the phases of maternity in the province receiving good scores. Among the benefits of providing this care, some cases such as reducing pain, decreasing anxiety, and increasing the rate of spontaneous delivery can be mentioned27. One of the main issues in this area is closely monitoring and midwife’s attendance at the woman-in-labor bedside, which is the most important emotional support. The continuous presence of midwife is as important as its quality, and maintaining such a relationship leads to confidence and tranquility of women, reinforcing mothers’ body for the production of endorphins28. The results of a study by Gagnon et al. showed that the presence of a caregiver for each woman during childbirth significantly reduced the use of oxytocin and subsequent obstetric complications29. Considering Iran, the presence of husband is not possible during childbirth, but emotional support in Lorestan health centers was desirable.
In the second stage, it is recommended that heart rate be controlled every fifteen minutes in low-risk deliveries, and every five minutes in high-risk pregnancies2,24. The results also confirmed the implementation of guidelines offered by the World Health Organization in this field. One of the important measures in the progression of the second stage of childbirth is preparing mothers and training them for cooperation30. This measure had good quality in the medical centers of the province.
Episiotomy is one of the actions performed in the treatment centers of the province with good quality. However, nowadays, the desire for episiotomy is decreased due to side effects, including fecal incontinence; therefore, it must be used in the elections having fetal indications such as shoulder dystocia, breech delivery, using forceps and vacuum, etc.31. It is assumed that the service providers of the province need more in-service training to meet new relevant research results and guidelines.
In the third stage of childbirth, newborn examination and blood pressure control had moderate quality and achieved less than 67% of the total score. Regarding the importance of newborn examination in the first hour for the fast identification of fetal abnormalities and gaining basic information for subsequent examinations, sufficient attention has not been devoted to this issue in the health centers of the province; thus, it needs to be promoted. Blood pressure control is one of the basic measures to assess the mother’s health during childbirth, predict and diagnose disorders such as dangerous postpartum hemorrhage23. According to numerous studies, hemorrhage is one of the main causes of maternal death during pregnancy and childbirth, which can be prevented by diagnosis and timely interventions5. Hypotension is an early sign of hidden bleeding. Therapeutic interventions can be performed by the exact control of hypotension, thus, preventing further complications. However, the results indicate that this issue has moderate quality in Lorestan health centers and needs upgrading to serve as a step towards improving maternal health.
Based on the results, the quality of care during childbirth in many fields, especially in the critical care fields discussed, were moderate or optimal and only in a few fields, the quality was poor. According to the above discussion, the weaknesses are in those issues, which somewhat lost their importance due to the replacement of new equipment and thus have received little attention by care providers, or issues like blood pressure. It is necessary to investigate causes and solutions for these issues.
In this study, an assessment tool was constructed for measuring the quality of care in different stages of childbirth according to the guidelines of the Iranian Ministry of Health, Treatment, and Medical Education. According to the results, it is recommended that the following measures be adopted: more training courses on the practical skills of maternity wards; installation of the protocols of the Ministry in the health centers; promotion of partograghy usage and acquaintance of the staff with this method; critical need for sensitization of employees to perform simple, but important care such as pulse control and hand washing while conducting surveillance; better communication with patients as well as preparing and introducing them with the delivery environment with more satisfaction; and improving the quality of care.
The results of the quality part showed that the university authorities were aware of many health care fields including ways of enhancing the quality and welcoming in-service training, use of on-call midwife (i.e. midwife for newborn care), improving the quality of the physical environment of the hospital and standardization of the midwife ratio to childbirth in the province. During the two-year research project, major initiatives have been taken in these fields. The authorities did not approve some of the causes of the quality loss with documentation (such as lack of work force). According to the consensus of top authorities of the medical universities as well as maternity officials and midwives in areas such as expansion of physical space, increasing the quantity and quality of in-service training and assignment of responsibility to more specialized staff in the field of women’s care and practical measures in this field during recent years, it seems that this strategy can overcome shortcomings in some fields of care. It should be noted that during interviews with maternity staff and officials, tangible changes were observed in some fields such as examination of the newborn, primary care of the newborn, correct completion of the partograghy forms and supplying necessary equipment for hand washing in the maternity, which confirms the results of the quantitative part of the project and awareness of authorities concerning these problems and necessary measures to eliminate them.
CONCLUSION
Considering the quality of care during childbirth as intermediate in all four stages in the province and investigation of the reasons indicating the lack of sufficient incentive in midwives, it is recommended that strategies such as financial incentives, greater use of private sector to reduce public sector workload, quality increase and further use of in-service training to improve the quality of services be adopted.
ACKNOWLEDGEMENTS
The authors would like to appreciate the Research and Technology Deputy Offices of Lorestan and Isfahan Universities of Medical Sciences (for funding the project), Isfahan School of Nursing and Midwifery, as well as vice-chancellor of Lorestan University of Medical Sciences for their cooperation in this project.
Author Disclosures:
Authors Changaei F., Simbar M., Irajpour A. and Akbari S. have no conflicts of interest or financial ties to disclose.
Corresponding Author:
Farahnaz Changaei
Department of Nursing and Midwifery,
Isfahan University of Medical Sciences,
Isfahan, Iran
E-mail:






