
Authors: Gülin Köseoğlu1*, Denada Haka1, Murathan Ekent2, Nedim Çekmen2
1MD, Anesthesiology
2MD, PhD, Anesthesiology
1Department of Anesthesiology and Intensive Care Unit, Baskent University, Faculty of Medicine Ankara, Turkey
*Correspondence: Baskent University, Faculty of Medicine, Department of Anesthesiology and Intensive Care Unit, Ankara, Turkey, Email: , GSM:+905304573934,
Tel: 0312203 68 68-4867
ABSTRACT
Conn’s syndrome is characterized by excessive aldosterone secretion, which can also occur due to an adrenal adenoma or adrenal hyperplasia. Conn’s syndrome is a prevalent cause of secondary hypertension characterized by excessive aldosterone secretion, resulting in Na+ retention, hypokalemia, and resistant hypertension. We aimed to present the successful anesthesia management of a 40-year-old female patient with severe hypokalemia, hypertension, and muscle cramps who underwent laparoscopic adrenalectomy due to Conn’s syndrome, due to a left adrenal adenoma. We emphasize the importance of comprehensive preoperative evaluation, a multidisciplinary approach, personalized patient management, and ensuring electrolyte imbalance and hemodynamic stability in the perioperative period.
INTRODUCTION
Primary hyperaldosteronism, also known as Conn syndrome, is characterized by autonomous aldosterone secretion from the adrenal cortex and is usually due to an adrenal adenoma or bilateral adrenal hyperplasia, resulting in suppression of plasma renin activity1-3. While Conn syndrome is seen in 5-10% of all hypertensive patients, this rate is around 20-25% in those with resistant hypertension3. Increased aldosterone secretion results in Na+ and water retention by the kidneys and increased excretion of potassium (K+) and H+ ions. These pathophysiological mechanisms lead to hypertension, hypervolemia, hypokalemia, and metabolic alkalosis, especially manifesting clinically as hypertension and hypokalemia. Suppressed plasma renin activity is a hallmark diagnostic feature4,5. Surgical intervention is generally indicated in cases of an aldosterone-producing adenoma4. Anesthetic management in Conn’s syndrome presents considerable challenges due to persistent hypertension, the risk of arrhythmias induced by hypokalemia, and altered responses to neuromuscular blocking agents6. The mechanism and treatment of Conn syndrome are outlined in Table 1.
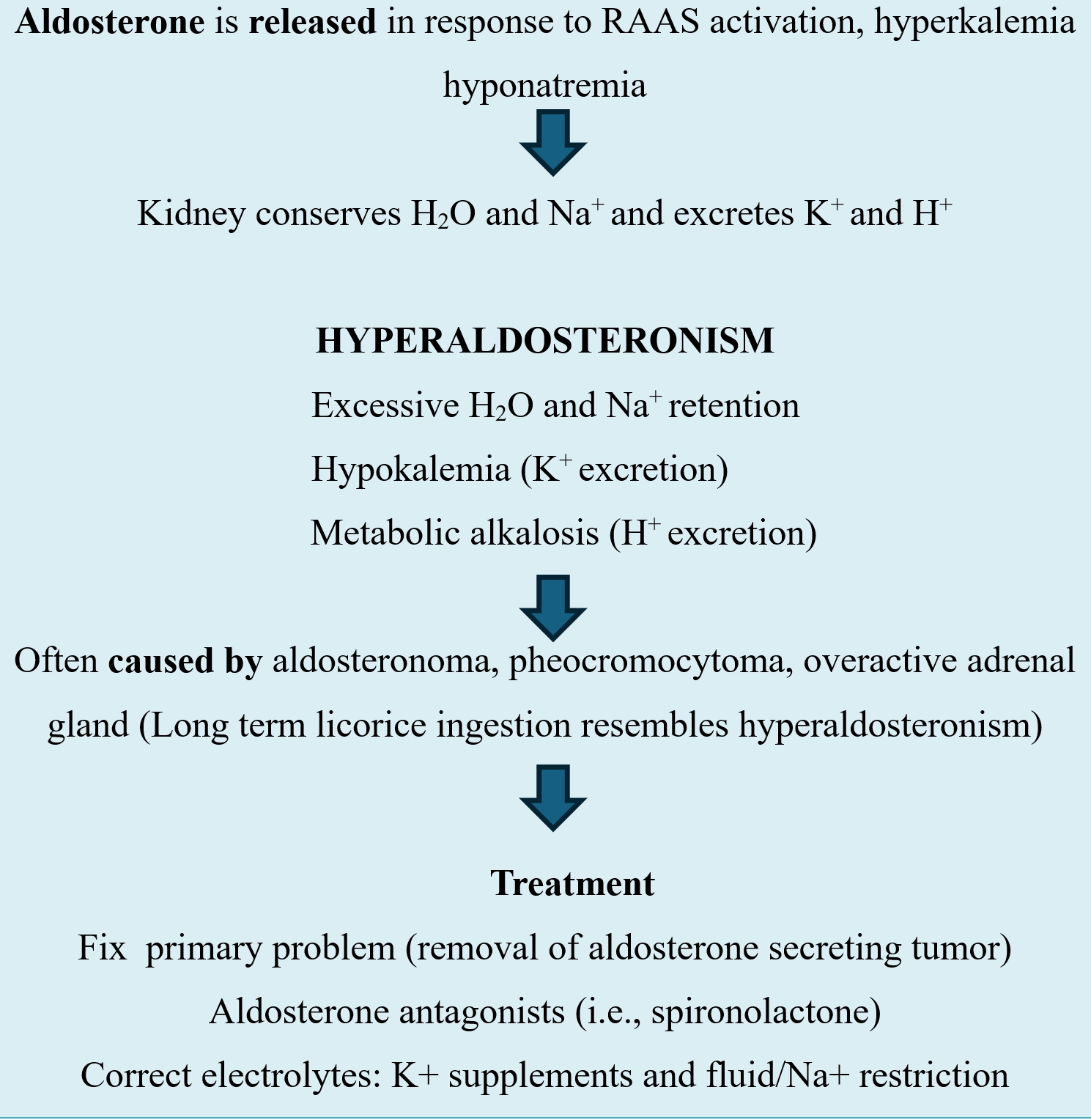
Table 1. The Mechanism and Treatment of Conn Syndrome
Herein, in our case, we present the successful anesthetic management of a 40-year-old woman who underwent laparoscopic adrenalectomy due to Conn syndrome secondary to a left adrenal adenoma and presented with severe hypokalemia, hypertension, and muscle cramps.
CASE PRESENTATION
A 40-year-old female (height 1.55 m, body weight 105 kg, and BMI 43.75 kg/m²) prese-nted with hypertension, hypokalemia, fatigue, muscle cramps, and generalizedweakness. A computed tomography (CT) scan revealed a left adrenal adenoma (Figure 1), and she was planned for a left-sided laparoscopic adrenalectomy.
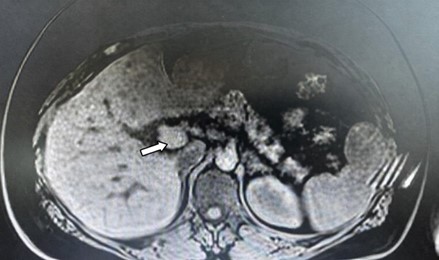
Figure 1. Patient’s computed tomography (CT) scan demonstrating a left adrenal adenoma (arrow).
On physical examination, her blood pressure (BP) was 180/100 mmHg. Laboratory tests are detailed in Table 2. The electrocardiogram (ECG) showed a heart rate (HR) of 54 beats per minute. A transthoracic echocardiography showed normal left ventricular wall thickness and preserved diastolic function with an ejection fraction of 53%.
| Laboratory Values | Value | Reference Range |
| Hemoglobin (g/dL) | 11.1 | 12–16 (female) |
| Hematocrit (%) | 34.2 | 36–46 (female) |
| Glucose (mg/dL) | 207 | 70–110 (fasting) |
| Potassium (K+) | 2.6 | 3.5-4.5 |
| Sodium (Na+)(mEq/L) | 143 mEq/L | 135-145 |
| Creatinine (mg/dL) | 0.8 mg/dL | 0.5-1 |
| Blood urea nitrogen (mg/dL) | 13 mg/dL | 6-20 |
| Plasma renin activity (ng/mL/hr) | 0.1 | 0.1-6.56 |
| Aldosterone (ng/mL) | 472 | 35-300 |
Table 2. Laboratory Values
Abdominal ultrasonography identified hepatic steatosis, and both kidneys exhibited normal size, parenchymal thickness, and echogenicity. The right adrenal gland appeared normal, whereas a 21×15 mm lesion was noted in the left adrenal gland (Figure 1). The patient was on antihypertensive therapy including nifedipine 30 mg twice daily, doxazosin 4 mg once daily, and nebivolol 5 mg once daily. Potassium (K+) supplementation was continued with tablets containing 2 grams of potassium bicarbonate and 2.17 grams of potassium citrate, administered twice daily. She had discontinued spironolactone treatment eight months prior. Venous aldosterone sampling was unsuccessful due to technical difficulties during catheterization. The 1 mg dexamethasone suppression test showed adequate cortisol suppression. Twenty-four-hour urine meta-nephrine and normetanephrine levels were normal. Aldosterone suppression was not observed after saline infusion testing. Based on these findings, a diagnosis of primary hyperaldosteronism was made, and surgical treatment was planned.
The patient exhibited non-adherence to oral K+ supplementation. Therefore, during pre-operative optimization two days prior to the scheduled surgical procedure, initiation of intravenous (IV) K+ replacement was necessary. Initial laboratory evaluation revealed a serum K+ level of 2.6 mEq/L. To correct the hypokalemia, three ampoules of potassium chloride, each containing 0.75 g (≈10 mEq), totaling 30 mEq, were administered at an infusion rate of 10 mEq/hour, after which a control measurement was obtained. The serum K+ level increased to 2.9 mEq/L following replacement. The following day, a similar total dose (30 mEq) of IV replacement was planned; however, pre-infusion assessment demonstrated a K+ level of 2.7 mEq/L. After administration using the same protocol, the K+ level rose only to 3.0 mEq/L. To correct refractory hypo-kalemia by addressing the underlying hypomagnesemia, the patient received magne-sium sulfate replacement at 12 mEq, admi-nistered twice daily on the first and second days, for a total of 4 doses. The trend of the measured K+ levels is presented in Table 3. Failure to achieve target levels despite consecutive and adequate IV K+ replacement suggested refractory hypokalemia. Following these interventions, the patient’s electro-cardiogram showed no repolarization abnormalities or arrhythmic events attributable to hypokalemia. With hemodynamic parameters remaining stable and the limited response to electrolyte optimization, the decision was made to proceed with the surgical intervention.
The patient’s American Society of Anesthesiologists physical classification is III, and the patient has a Mallampati score of II. The verbal and written consent was obtained from the patient for the publication of this case report.
| Time Point | Serum K+ Levels (mmol/L) |
| Preoperative Evaluation | 2.6 |
| 2 days preoperatively (before replacement) | 2.6 |
| 2 days preoperatively (after replacement) | 2.9 |
| 1 day preoperatively (before replacement) | 2.7 |
| 1 day preoperatively (after replacement) | 3.0 |
| At surgery onset | 2.7 |
| At surgery completion | 3.1 |
Table 3. Serum K+ Levels (mmol/L) during the Perioperative Period
In the operating room, the patient was connected to standard monitoring, including ECG, noninvasive blood pressure (NIBP), pulse oximetry (SpO₂), end-tidal carbon dioxide (EtCO₂), and a train-of-four (TOF) monitor for continuous neuromuscular monitoring. A central venous catheter was inserted, and a 16-gauge IV cannula was placed for volume replacement, and a left radial arterial catheter was inserted for invasive blood pressure monitoring. At the beginning of the procedure, the patient’s HR was 75 bpm, NIBP was 175/100 mmHg, and SpO₂ was 98%. The patient was premedicated with 0.01 mg/kg midazolam IV. Anesthesia induction was carried out with propofol, fentanyl, and rocuronium bromide as a neuromuscular blocker. The patient was intubated with a 7.5 mm endotracheal tube without any compli-cations. Anesthesia was maintained throughout the procedure using a 50% oxygen–50% air mixture, 2.2% sevoflurane, and a remifentanil infusion at 0.05–0.1 mcg/kg/min. 100 mg hydrocortisone was administered IV for its anti-inflammatory effects, to support cardiovascular stability, and to reduce the risk of adrenal insufficiency. The patient was in volume-controlled mode, and positive end-expiratory pressure (PEEP) was set at 4-6 cmH₂O. The patient’s PEEP was maintained at a relatively high level to prevent complications related to pneumoperitoneum, which can occur during laparoscopic abdominal surgeries. During surgery, the patient’s BP ranged between 130–180 mmHg systolic and 60–95 mmHg diastolic. Intravenous fluid therapy consisted of Plasmalyte and colloid solutions for preventing hypovolemia. The patient’s blood gas results were analyzed and are presented in Table 4.
The K+ levels fluctuated between 2.7 and 3.1 mEq/L. The K+ replacement was administered at 10 mEq/hour, totaling 20 mEq during the two-hour laparoscopic left adrenalectomy. Due to refractory hypokalemia, the patient was administered 12 mEq of magnesium sulfate twice.
However, there was no response to K+ replacement, and serum K+ levels could not be corrected to the desired range. Total surgical duration was 120 minutes. The procedure resulted in approximately 350 mL of blood loss, with no requirement for blood products. After postoperative hemostasis control, the surgery was completed without incident. The surgical specimen (Figure 2) was sent for pathologic examination.
| Laboratory Values | Result | Result | Reference Range |
| pH | 7.467 | 7.44 | 7.35–7.45 |
| PaCO₂ (mmHg) | 37 | 41 | 35–45 |
| PaO₂ (mmHg) | 81.5 | 84.3 | 75–100 |
| SaO₂ (%) | 96.4 | 97.7 | 94–98 |
| Na⁺ (mmol/L) | 134 | 138 | 135–145 |
| K⁺ (mmol/L) | 2.7 | 3.1 | 3.5–5.0 |
| Ca²⁺ (mmol/L) | 0.98 | 1.05 | 1.12–1.32 |
| Lactate (mmol/L) | 0.90 | 0.95 | 0.5–2.2 |
| Glucose (mg/dL) | 207 | 190 | 70–110 (fasting) |
| Hemoglobin (g/dL) | 11.1 | 11.0 | 12–16 (female) |
| Hematocrit (%) | 34.2 | 34 | 36–46 (female) |
| HCO₃⁻ (mmol/L) | 26.4 | 26 | 22–26 |
| Base Excess (BE) (mmol/L) | 3.1 | 3.0 | –2 to +2 |
Table 4. Periopetaive values of Arterial Blood Gas and Biochemical Parameters.
Figure 2. Laparoscopic view of left adrenal mass.
In the postoperative period, 1000 mg paracetamol was administered as an analgesic, and 3 mg granisetron was administered for nausea and vomiting. After 200 mg of sugammadex was administered for neuromuscular antagonism, the patient was extubated and transferred to the intensive care unit for close observation. On follow-up, the patient’s potassium levels and clinical condition remained stable, and she was discharged 4 days after surgery.
DISCUSSION
In our case, we highlight the complex challenges anesthesiologists face in managing Conn’s syndrome patients. In Conn’s syndrome, excessive aldosterone secretion increases Na+ reabsorption in the renal tubules, leading to water reabsorption, increased total blood volume, and refractory hypertension1-3. As Na+ reabsorption increases, K+ and H+ are released, resulting in refractory hypokalemia (serum K+ < 3.5 mEq/L) and alkalosis despite oral K+ supplements3-6. Our patient had complaints of hypertension, hypokalemia (2.6 mEq/L), muscle cramps, fatigue, and generalized weakness.
Anesthetic management in patients with Conn’s syndrome undergoing adrenalectomy requires careful preoperative optimization of persistent hypokalemia, labile BP, and metabolic alkalosis to reduce the risk of perioperative cardiovascular complications5,6. Hypokalemia prolongs the effects of non-depolarizing neuromuscular blocking agents6, and therefore, we used TOF. Hypokalemia can lead to arrhythmias because it depresses baroreceptor tone, and therefore, hypokalemia should be treated aggressively in the perioperative period6..Hypertension treatment requires a combination of several drugs to regulate BP, depending on comorbidities and complications. The first-line therapeutic agent is spironolactone, a K+-sparing diuretic administered (100–400 mg/day). Alternatively, amiloride or nifedipine (30–90 mg/day), 5–15 mg/day, and angiotensin-converting enzyme (ACE) inhibitors (captopril) and angiotensin receptor inhibitors (losartan-Na+) can also be used2,4,6. In our case, maintaining normokalemia despite aggressive K+ replacement and maintaining BP control despite multiple antihypertensive agents (Esmolol and nitrate) proved challenging.
Hypovolemia, which develops as a result of hypokalemia suppressing baroreceptor tone and a combination of other factors such as antihypertensives (ACE inhibitors) and diuretics, anesthetic drugs, positive pressure ventilation, and laparoscopic insufflation, should be treated aggressively4,6. In our patient, the antihypertensive drugs were stopped on the morning of surgery, and the patient’s hemodynamics were monitored with invasive monitoring and stabilized by maintaining adequate depth of anesthesia with anesthetic agents such as sevoflurane and remifentanil, volume replacement with IV crystalloids and colloidal fluids during the operation. During surgery, hemodynamic fluctuations can occur frequently due to sudden changes in circulating aldosterone and catecholamine levels, which are often triggered by surgical manipulations. Agents such as esmolol, phentolamine, nitro-glycerin, and norepinephrine were available throughout the surgery to manage sudden hemodynamic fluctuations. In our case, mini-mal hemodynamic fluctuations were noted during surgical manipulation.
In laparoscopic surgeries, venous return and lung compliance are reduced by raised intra-abdominal pressure (IAP) and hypercarbia induced by pneumoperitoneum, leading to significant changes in ventilation, oxygenation, and hemodynamics7. Therefore, we tried to keep our patient’s IAP at 14 mmHg, the patient’s position, and avoid hypercarbia.
Ravi R et al.8 reported that a 36-year-old patient with hypokalemia, hypertension, and muscle cramps who underwent right-sided laparoscopic adrenalectomy developed severe hypotension following pneumoperitoneum, requiring fluid replacement and vasopressors. Kharat PA et al.9 reported that the perioperative course of a 37-year-old patient with right adrenal adenoma, quadriparesis, malignant hypertension, hypokalemia, metabolic alkalo-sis, rhabdomyolysis, and high aldosterone levels who underwent laparoscopic adrenale-ctomy under general anesthesia was uneventful. Latha YS et al.10 reported that no problems other than a hypotension episode were encountered during laparoscopic adrenalectomy surgery in a 51-year-old patient with Conn syndrome who had hypertension, generalized muscle weakness, and hypoka-lemia. Our patient’s hemodynamics remained stable, but the most important intraoperative problem encountered in our patient was persistent hypokalemia resistant to treatment.
CONCLUSION
Patients with Conn’s syndrome present a significant challenge for anesth-esiologists due to persistent hypertension and hypokalemia. Careful and vigilant periope-rative hemodynamic monitoring and correction of electrolyte and metabolic abnormalities are crucial to their successful management. A multidisciplinary team approach, including anesthesiologists, endocrinologists, and surge-ons, is essential for meticulous perioperative monitoring.
Addittional materials: No
Acknowledgements: Not applicable
Authors’ contributions: GK: data collection, planning, literature review, manuscript preparation, final draft, is the lead author, DH: literature review, manuscript preparation, critical review, ME: literature review, manuscript preparation, critical review, NÇ: supervision, critical review. All authors read and approved the final manuscript..
Funding: Not applicable.
Ethical approval and consent to participate: No IRB approval required. Inform consent was obtained.
Competing interests: The authors declare that they have no competing interests.
Received: November 2025, Accepted: December 2025, Published: March 2026.
REFERENCES
- Hundemer GL, Vaidya A. Primary Aldosteronism Diagnosis and Management: A Clinical Approach. Endocrinol Metab Clin North Am 2019;48(4):681-700. doi:10.1016/j.ecl.2019.08.002.
- Faconti L, Kulkarni S, Delles C, et al. Diagnosis and management of primary hyperaldosteronism in patients with hypertension: a practical approach endorsed by the British and Irish Hypertension Society. J Hum Hypertens 2024;38(1):8-18. doi:10.1038/s41371-023-00875.
- Monticone S, Burrello J, Tizzani D, et al. Prevalence and Clinical Manifestations of Primary Aldosteronism Encountered in Primary Care Practice. J Am Coll Cardiol 2017;69(14):1811-20. doi:10.1016/j.jacc.2017.01.052.
- Mulatero P, Monticone S, Burrello J, et al. Guidelines for primary aldosteronism uptake by primary care physicians in Europe. J Hypertens 2016;34(11):2253-7. doi:10.1097/HJH.0000000000001088.
- Citton M, Viel G, Rossi GP, et al. Outcome of surgical treatment of primary aldosteronism. Langenbeck’s Arch Surg 2015;400(3):325-31. doi:10.1007/s 00423 -014-1269-4.
- Domi R, Sula H, Kaci M, et al. Anesthetic considerations on adrenal gland surgery. J Clin Med Res 2015;7(1):1-7. doi:10.14740/jocmr1960w.
- Atkinson TM, Giraud GD, Togioka BM, Jones DB, Cigarroa JE. Cardiovascular effects of laparoscopic surgery. Circulation 2017;135(7):700-10.
- Ravi R, Prabhu M, Vamadevan BT. Anesthetic Implications in Managing a Case of Primary Hyperaldosteronism: A Case Report. Cureus 2023;15(2):e35502. doi:10.7759/cureus 35502.
- Kharat PA, Dalvi NP, Bagde T, et al. Anesthesia Considerations of a Case of Conn Syndrome. J Research and Innovation in Anesthesia 2022;7(1):22-24. doi.org/10.5005/jp-journals-10049-2005.
- Latha YS, Bhatia N, Arora S. Perioperative management of Conn’s syndrome – a case report. Anaesth, Pain & Intensive Care 2014; 18(2):204-6.
Publisher’s Note
The publisher remains neutral with regard to jurisdictional claims in published maps and institutional afliations.
| Citation: Gülin Köseoğlu, Denada Haka, Murathan Ekent, Nedim Çekmen. Successful Anesthesia Management in a Patient with Refractory Hypokalemia and Hypertension Due to Conn Syndrome Undergoing Laparoscopic Adrenalectomy: A Case Report. Greek e j Perioper Med. 2026;245(a): 47-56. |






