
Authors: Volakli EMD, PhD, Sdougka MMD, Mantzafleri PE, MD, Tsonidis Ch MD, PhD, Kontopoulos E MD, PhD, Tsikoulas I MD, PhD.
ABSTRACT
The goal of of the present study is to investigate short-term and long-term functional outcome of a 8-bed, multidisciplinary pediatric intensive care unit (PICU) of a general hospital 300 PICU patients were enrolled prospectively in this observational cohort study. Functional outcome was evaluated through Pediatric Cerebral Performance Category (PCPC) and Pediatric Overall Performance Category (POPC) scales at admission (baseline), at PICU and hospital discharge, at 3 and 6 months, and at 1 and 2 years. Delta DPCPC and DPOPC alterations at discharge were related to major diagnostic categories and 2-year survival.Baseline PCPC and POPC scores were normal in 67% and 58.7% of study population, mild disability were recorded in 17.3% and 14.7%, moderate disability at 8% and 14%, severe disability at 4.3% and 9.3% and coma at 3.3% and 3.3%, respectively. At two years, normal PCPC and POPC scores were found in 66% and 47% of patients, mild disability in 17.3% and 30.5%, moderate disability in 9.5% and 13.6%, severe disability in 2.9% and 4.9% and coma in 4.1% and 4.1%, accordingly. Two years after discharge patients reached their PCPC baseline categories but lacked behind in POPC categories (p=0.001). Best functional outcome at discharge was recorded in respiratory and postoperative patients followed by cardiovascular, neurologic and trauma patients. Statistically significant differences were found in 2-year survival according to DPCPC [χ2 (2)=77.77, p<0.001] and DPOPC categories [χ2 (2)=44.66, p<0.001]. In conclusion, we found that two years following PICU discharge functional outcome parameters approached their preadmission values. Therefore, this chosen time period seemed to be adequate for studying long-term outcome of pediatric intensive care. Long-term PICU survivors had satisfactory PCPC (92.8%) and POPC (91.1%) categories to live an independent life. The impact of critical illness was greater on overall performance than in cognitive function.
INTRODUCTION
The aim of the Pediatric Intensive Care Unit (PICU) is the close observation and monitoring, as well as the optimal care and improved outcome of the patients. Severity-adjusted mortality at PICU discharge is the main short-term outcome tool and the general perception is that PICU mortality rate is quite low with the reported values being less than 6%1-5. Apparently, long-term mortality two to three years following PICU admission is much higher (up to 20%), as mentioned be several investigators6-12. Moreover, survivors often experience various degree of morbidity after discharge leading them to multiple hospital and PICU admissions. Therefore, it is crucial to supply short-term and long-term morbidity data to provide an integrated outcome assessment of pediatric intensive care.
Morbidity studies in PICU survivors suffer from small numbers, subgroup evaluations, methodological limitations, quantitative and qualitative heterogeneity, short follow-up periods and follow-up losses that complicate the interpretation of the data13-16. Some of them focus on functional outcome which can be evaluated more objectively, whereas others assess more subjective aspects of quality of life. Additionally, chronic conditions should be taken into account in order not to overlook unrecognized health deficits that are important to the outcome of critical illness5,17. The reported favored functional outcome and/or quality of life in cohorts of PICU survivors two to 3.5 years after discharge range from 59.3% to 91% 6, 8-9,18.
Pediatric Cerebral Performance Category (PCPC) and Pediatric Overall Performance Category (POPC) scales were developed by D. Fisher to measure easily and quantify effectively morbidity after a child’s critical illness or injury19. PCPC focuses on cognitive impairment whereas POPC focuses on functional morbidity and both are well associated to more comprehensive and well-established psychometric measures of functioning. They are valid and reliable tools that have been further evaluated in large multi-institutional studies20,21, and are considered as references to newer functional outcome measures 19,22.
The primary objective of the present study was to describe short-term and long-term functional outcome of PICU patients using PCPC and POPC scales at admission and during a two years longitudinal follow-up period. Until now, PCPC and POPC scales were used in cohorts of PICU patients only during the first three months following PICU discharge; in our study we extended the follow-up period to 2 years to investigate whether and when the patients return to their previous functional status. The secondary objective was to examine if the alterations of PCPC and POPC scores at PICU discharge, estimated as delta DPCPC and DPOPC scores, were related to major diagnostic groups and the 2-year survival.
MATERIAL AND METHODS
Participants. Prospective observational cohort study of 300 critical care pediatric patients, aged older than 40 days up to 14 years, admitted between 2001 and 2004 in a multidisciplinary, tertiary, 8-bed Greek PICU. All diagnostic categories were included, except postoperative heart surgery patients. Exclusion criteria: readmissions, patients who died during the first two hrs of admission, and patients with missing data throughout the study period. The study was approved by the Institutional Ethical and Scientific Committee and informed consent was obtained from the parents or guardians ofthe patients. Follow-up was done with personal patient contact until hospital discharge and bytelephone interviews at 3 and 6 months and at 1 and 2 years afterward, by the principal investigator.
The full description of PCPC and POPC scales are analyzed in Tables 1 and 2.
| Score | Category | Description |
| 1 | Normal | At age appropriate level; school-age child attend regular school |
| 2 | Mild disability | Conscious, alert, able to interact at age-appropriate level; regular school, but grades perhaps not age-appropriate, possibility of mild neurologic deficit |
| 3 | Moderate disability | Conscious, age-appropriate independent activities of daily life; special education classroom and/or learning deficit present |
| 4 | Severe disability | Conscious, dependent in others for daily support because of impaired brain function |
| 5 | Coma or vegetative state | Any degree of coma, unaware, even if awake in appearance, without interaction with the environment; no evidence of cortex function; possibility for some reflexive response, spontaneous eye-opening, sleep-wake cycles |
| 6 | Brain death/death | Brain death, death |
Data collection. Demographics, admission related status, selected critical care modalities, and the outcome at the above time intervals were recorded prospectively. Severity of critical illness was estimated through the Pediatric Risk of Mortality (PRISM III-24)1. PCPC and POPC scales were retrospectively evaluated at admission as baseline values, and subsequently at the predefined longitudinal follow-up periods; at PICU and hospital discharge, at 3 and 6 months, and at 1 and 2 years.
| Score | Category | Description |
| 1 | Good overall performance | PCPC 1; healthy, alert, and capable
of normal activities of daily life |
| 2 | Mild overall disability | PCPC 2; possibility of minor physical problem that is still compatible with normal life |
| 3 | Moderate overall disability | PCPC 3; possibility of moderate disability from non cerebral systems dysfunction aloneor with cerebral dysfunction; performs independent activities of daily life but disabled for competitive performance at school |
| 4 | Severe overall disability | PCPC 4; possibility of severe disability from non cerebral systems dysfunction alone or with cerebral dysfunction; conscious but dependent on others for activities of daily living support |
| 5 | Coma or vegetative state | PCPC 5 |
| 6 | Brain death/death | PCPC 6 |
PCPC, Pediatric Cerebral Performance Category; POPC, Pediatric Overall Category Scale; POPC is dependent on PCPC scale as a result of inclusion of PCPC status in the operational definitions of the POPC scale categories.
Statistical analysis. Discrete variables were expressed as counts (percentages) whereas continuous variables as median (interquartile range). Comparisons of PCPC and POPC categories at admission with the values obtained at the study intervals were tested by Kruskal-Wallis nonparametric test. Delta DPCPC and DPOPC scores were calculated by subtracting the admission from the discharge score. Due to relatively small study size, three groups were assigned as follows: group 0 = no decline, group 1 = 1 category decline, group 2 = 2 to 5 categories decline, and their relationship to major diagnostic groups were sought by chi-square test. Two year survival data were analyzed with standard Kaplan-Meier technique and the impact of DPCPC and DPOPC alterations at discharge on survival were explored using the log-rank test. Data were analyzed using SPSS 11.0 for windows (SPSS, Chicago, IL). A p<0.05 was considered statistically significant.
RESULTS
Among 382 consecutive admissions, 300 patients (196 boys and 94 girls), aged 36 (11-96) months, completed the 2-year follow-up period and were included in the study (Figure 1).
The overwhelming majority were emergencies (92.3%) that were admitted from referral hospitals (68%), either in town (27%) or from remote geographical areas (41%).
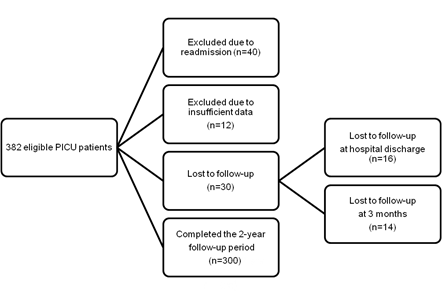
Figure 1. Study flow chart
Most patients had an excellent health status prior PICU admission, but quite a lot (41.3%) suffered from co-morbidities. Neurologic failure (23.3%), respiratory failure (22.3%), trauma (22.3%), cardiovascular failure/shock (10%), postoperative care (7.7%) and other miscellaneous diseases (14.5%) represented the main reasons for admission.
Median PRISM III-24 score was 7 (3-11). Mechanical ventilation (MV) rate was 67.3% (58.3% at admission) and MV duration was 2.5 (1-6.25) days. Patients stayed in the PICU for 4 (2-8) days and hospitalization lasted 12 (7-23) days. PICU, hospital, 3-month, 6-month, 1-year and 2-year cumulative mortality rates were 9.7%, 12.7%, 15%, 16.7%, 19%, and 19%, respectively.
PCPC and POPC categories at admission and during the follow-up period are exposed in Tables 3 and 4.
An enormous decline in functional outcome was recorded at PICU discharge; only 21% of our patients had intact cerebral function and the proportion dropped further down to 0.7% for normal overall performance. After discharge, there was an improvement in PCPC and POPC categories, as expected during recovery of critical illness.
| Patients, n (%) | |||||||
| PCPC score | Admission (baseline) |
PICU dis-charge |
Hospital dis-charge |
3 m | 6 m | 1 yr | 2 yrs |
| 1 | 201 (67.0) |
63 (21) |
118 (44) |
141 (54) |
147 (58) |
154 (62) |
161 (66) |
| 2 | 52 (17.3) |
120 (40) |
74 (27) |
51 (19.5) |
50 (19.6) |
44 (17.6) |
42 (17.3) |
| 3 | 24 (8.0) |
38 (12.7) |
32 (12) |
31 (11.8) |
26 (10.2) |
27 (10.8) |
23 (9.5) |
| 4 | 13 (4.3) |
33 (11) |
21 (7.7) |
19 (7.3) |
15 (5.9) |
8 (3.2) |
7 (2.9) |
| 5 | 10 (3.3) |
17 (5.7) |
17 (6.3) |
13 (5) |
12 (4.7) |
10 (4.0) |
10 (4.1) |
| 6 | 0 (0.0) |
29 (9.7) |
9 (3.0) |
7 (2.3) |
5 (1.7) |
7 (2.3) |
NA |
| Pts | 300 | 271 | 262 | 255 | 250 | 243 | 243 |
| p* | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | ns | |
PCPC, Pediatric Cerebral Performance Category; PCPC scores: 1 normal; 2 mild disability; 3 moderate disability; 4 severe disability; 5 coma/vegetative state; 6 brain death/death; NA, not applicable; Pts: Patients; *Kruskal-Wallis test, compared to admission
Differences in PCPC and POPC categories at the study intervals compared to baseline values evaluated at admission were significant in each follow-up period, till a year after discharge (p<0.001).
PCPC categories approached their baseline values at two years (p>0.05). On the contrary, differences in POPC categories insisted even after two years following pediatric intensive care (p<0.001). At PICU discharge DPCPC and DPOPC group 0 consisted of 41.7% and 25% of patients, group 1 of 36.3% and 44.7%, and group 2 of 22% and 30.3%, respectively.
POPC, Pediatric Overall Performance Category; POPC scores: 1 good overall performance; 2 mild overall disability; 3 moderate overall disability; 4 severe overall disability; 5 coma/vegetative state; 6 brain death/death; NA, not applicable; Pts:Patients;*Kruskal-Wallis test, compared to admission
Patients, n (%)
POPC score
Admission
PICU discharge
Hospital dis-charge
3 m
6 m
1 yr
2 yrs
1
176
(58.7)2
(0.7)51
(18.8)79
(30)91
(36)102
(41)114
(47)
2
44
(14.7)127
(42.0)92
(33.9)77
(29)76
(30)77
(31)74
(30)
3
42
(14.0)69
(23.0)63
(23.2)60
(23)50
(19)39
(15)33
(13)
4
28
(9.3)56
(18.7)39
(14.4)26
(9.9)21
(8.2)15
(6)12
(4.9)
5
10
(3.3)17
(5.7)17
(6.3)13
(5.0)12
(4.7)10
(4)10
(4.1)
6
0
(0.0)29
(9.7)9
(3.0)7
(2.3)5
(1.7)7
(2)NA
Pts
300
271
262
255
250
243
243
P*
0.001
0.001
0.001
0.001
0.001
0.001
Alterations of DPCPC and DPOPC categories at PICU discharge according to major diagnostic groups are shown in Figure 2 and Figure 3. Respiratory and postoperative patients showed the best functional outcome; their cognitive function was even better than their overall performance, as the proportion of patients in DPCPC group 0 was significantly higher compared to groups 1, 2 (p<0.001) but the proportion of patients in DPOPC group 0 was significantly greater only compared to group 2 (p<0.05). On the contrary, trauma patients showed the worst cognitive and overall performance at PICU discharge as the proportion of patients that were found in DPCPC and DPOPC groups 0 were significantly lower compared to DPCPC and DPOPC groups 1 and 2 (p<0.01).
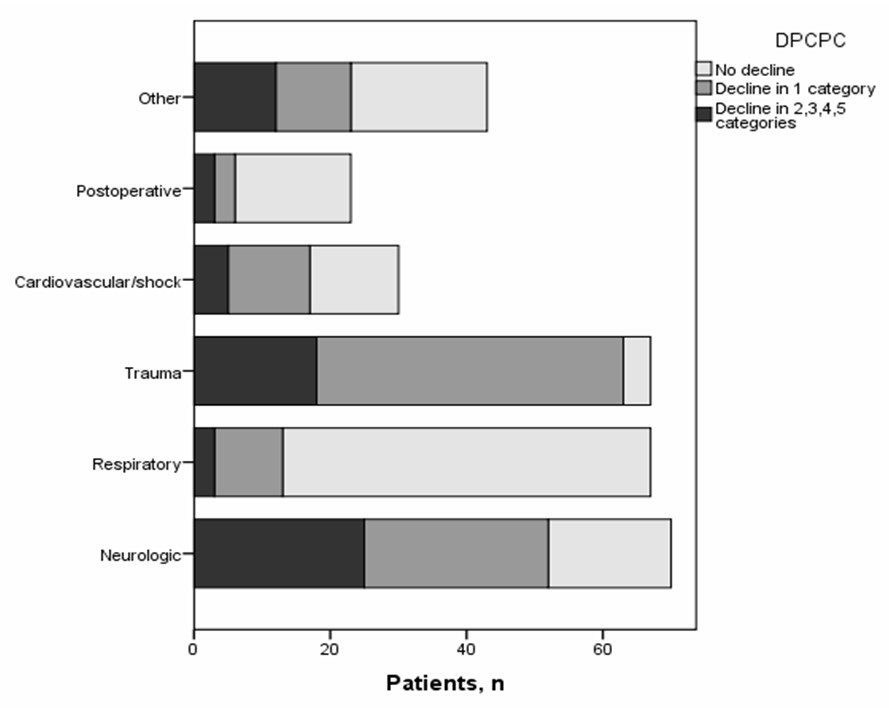
Figure 2. DPCPC categories at PICU discharge according to major diagnostic groups
DPCPC: Delta Pediatric Cerebral Performance Category calculated by subtracting the admission from the discharge score

Figure 3. DPOPC categories at PICU discharge according to major diagnostic groups
DPOPC: Delta Pediatric Overall Performance Category calculated by subtracting the admission from the discharge score
Cardiovascular patients experienced better cognitive function (more patients in DPCPC groups 0, 1 vs. group 2, p <0.05) compared to overall performance where no differences were found among the three groups (p>0.05). Alterations of DPCPC and DPOPC were equally distributed among the three groups in neurologic patients (p>0.05).
Kaplan-Meier estimates for 2-year survival in patients with different DPCPC and DPOPC groups at PICU discharge are given in Figure 4 and Figure 5.Statistically significant differences were found in 2 year survival according to DPCPC [χ2 (2) =77.77, p < 0.001] and DPOPC categories [χ2 (2) =44.66, p < 0.001]. Best survival was recorded in patients with one only category decline (DPCPC 1 and DPOPC 1) contrary to the worst outcome of patients with decline in more categories (DPCPC 2 and DPOPC 2), especially in the domain of cognitive function.

Figure 4. Kaplan-Meier estimates for 2-year survival in patients with different DPCPC categories
DPCPC: Delta Pediatric Cerebral Performance Category calculated by subtracting the admission from the discharge score. Log-rank test revealed statistical significance in survival curves [χ2 (2)=77.77, p < 0.001].

Figure 5. Kaplan-Meier estimates for 2-year survival in patients with different DPOPC categories
DPOPC: Delta Pediatric Overall Performance Category calculated by subtracting the admission from the discharge score. Log-rank test revealed statistical significance in survival curves [χ2 (2)=44.66, p < 0.001].
DISCUSSION
We assessed short-term and long-term functional status of PICU patients during a two years follow-up period to have an integrated assessment of their outcome. We found that two year following PICU discharge survivors had satisfactory PCPC (92.8%) and POPC (91.1%) categories to live an independent life. Respiratory and postoperative patients showed the best functional outcome whereas prognosis was worst for cardiovascular, neurologic and trauma patients. Survival was better for patients showing 1 only category decline in DPCPC and DPOPC scales at discharge, compared to patients with no decline or decline in more than one category.
We chose to use PCPC and POPC scales due to their broad use in cohorts of PICU patients.Original scales consisted of only five categories, whereas the pediatric versions have one additional category for mild disability with the premise that even mild functional impairment in children is significant because of its potential duration and impact on development. Both represent useful estimates of well-validated and comprehensive psychometric measures, on all age groups (infants included), and diagnostic categories (trauma included) and are ideal cohort functional outcome measures in a multidisciplinary setting. The evaluation of PCPC and POPC performance further than the three months that are reported in the literature enabled us to observe whether and when patients reached their preadmission functional status.
Short-term Pediatric Cerebral Performance Category Scale alterations:Normal cerebral baseline function was found in 67% of our patients, according to reference baseline values that range from 54% to 84.3%19,20, 23. More patients in our study were found in baseline coma/vegetative state status, probably due to the high proportion of admissions for neurologic reasons (23.3%). At PICU discharge fewer patients had intact cerebral function (21%) compared to the reported values of 40% to 58.4%20, 23. Our population characteristics, with the low percentage of postoperative patients and the high proportion of emergencies, neurologic and trauma patients, and the high severity of illness as reflected by the high severity score and the high proportion of MV, could explain our findings24. Like in the study of Morrison et al., respiratory and postoperative patients showed the best cerebral performance followed by cardiovascular patients8. On the contrary, cognitive dysfunction was higher in trauma patients, which is opposite to the before mentioned study. Neurologic patients showed a moderate outcome, similar to a relevant study18. Many patients in this group had preexisting deficits, and in those patients the impact of critical illness was less profound. From a clinical point of view, patients with moderate or severe disability or coma, even if survive will remain in the same low neurologic level of function.
At hospital discharge, less patients of our study had normal cerebral function and more patients had mild cognitive disability compared to the study of Fiser et al. (44% vs. 75.4% and 27% vs. 10.3%, respectively)19. We could attribute these discrepancies to the ongoing impact of the before mentioned reasons.
Long-term Pediatric Cerebral Performance Category Scale alterations:Three months after discharge 54% of our children had normal PCPC scores, a proportion lower than the reported (77%) by Knoester et al.14. Though, the previous investigators examined only children without known health problems at admission, where a better outcome is expected. Slower improvement rate was recorded at 6 months, 1 year and 2 years following discharge. There are not references using the same scale for the cognitive function of critically ill pediatric patients after the follow-up period of 6 months, so we will attempt to compare our findings to other outcome tools. Jones et al., estimating quality of life at 6 months, in PICU patients aged > 6 months using the Health Utility Index, found full health in 27.3% of children, a value that is lower than our results for normal cognitive function (35.7%)4.
One year after discharge normal cognitive performance was found in 62% of our patients compared to 72.6% of a related study7. Nevertheless, that study didn’t include infants and trauma (28.3% and 22.3 % in our study, respectively). Trauma is strongly related to worse cognitive and functional outcome in pertinent studies25,26 and the relative high proportion of our trauma patients could explain our findings. At two years, our population reached the baseline PCPC values. Normal PCPC scores were found in 66%, and mild disability in 17.3%. Both categories, together with patients with mild disability (9.5%) reached a population of 92.8% with good PCPC performance that is capable for independent life. In accordance to our results, good quality of life two to 3.5 years after pediatric intensive care range from 59.3% to 91%6, 8,9, 18.
Short-term Pediatric Overall Performance Category Scale alterations: Good baseline overall performance was found in 58.7% of our patients, slightly better than the reported values of 28.7% to 56.6%5,19,20,23. This probably reflected the high proportion of emergency patients (92.3% in our study) that didn’t suffer from impaired health status. Our finding approached the values of older studies whereas a more recent report showed that the fraction of patients that are admitted in a pediatric intensive care with a chronic condition increases over the decades of pediatric intensive care 5. The evolution of medicine in the field of neonatal intensive care and pediatrics, where more and more patients survive but at an expense of severe morbidity, could explain this finding12.
At PICU discharge an enormous decline in global function was recorded with a diminution of patients in POPC 1 to 0.7% compared to 14% up to 27.4% of relevant studies20-23. This finding is expected in previously healthy children when admitted in a PICU following an emergent high severity critical insult and experience the greatest decline in global function. Respiratory and postoperative patients showed also the best DPOPC performance compared to other diagnostic categories, but their effect was less profound compared to DPCPC performance. Trauma patients, once again, showed the worst overall performance whether cardiovascular and neurologic patients showed a moderate global outcome. Substantial improvement accompanied our patients at hospital discharge; however our data of normal POPC (18.8%) was lower than the reported ones of 30%19.
Long-term Pediatric Overall Performance Category Scale alterations: Good overall performance at 3 months was found in 30.2% of our patients, a value almost identical (31%) to that reported by Knoester et al.14. Six months after discharge good health status was found in 35.7% of our children, which was higher than the value (27.3%) reported by Jones et al.4. One year after discharge good overall performance was found in 41% of our study compared to 72.6% of a relevant study, which however didn’t include infants and trauma7. At two years, the percentage of patients with normal global function (47%) remained significantly lower compared to baseline, whether the proportion of patients with mild overall disability (30.5%) almost doubled. Though, those patients together with patients with moderate overall disability (13.6%) composed a proportion of 91.1% of POPC categories capable for independent life. Similar results for good quality of life two to 3.5 years after pediatric intensive care range from 59.3% to 91%, as already mentioned6, 8,9, 18.
Survival analysis:Survival analysis at 2 years showed that patients with more deficits at discharge, e.g., in DPCPC and DPOPD category 2, represented mostly from neurologic and trauma patients, had the worst outcome, especially in the domain of cerebral performance. This is an expected finding as the most impaired patients have less health reserves and is most possible to die. Interestingly, best outcome was found in patients with 1 category decline, which pictured previously healthy children, with only a limited deterioration due to critical illness. Patients without decline in functional outcome showed moderate results concerning long-term survival. Those patients represented children with known deficits at admission that were discharged at the same impaired health status. To our knowledge there is no study examining long-term survival according to alterations of functional status at PICU discharge to compare our results.
Limitations: This is a single center study and national differences concerning administration issues of pediatric intensive care pose barriers in the generalization of our results. However, the strict structured protocol of our study which included the evaluation of baseline functional status and the severity of illness, the zero follow-up losses and the long follow-up period enable us to add some more information in the field.
CONCLUSION
Our study is one of the few studies on the functional outcome in a cohort of PICU patients, and the unique using PCPC and POPC scales for such a long follow-up period. Two years after discharge functional outcome parameters approached their preadmission values. Therefore, this chosen time period seemed to be adequate for studying long-term outcome of pediatric intensive care. The majority of survivors had satisfactory PCPC (92.8%) and POPC (91.1%) categories to live an independent life. The impact of critical illness was greater on overall performance than on cognitive function. Pediatric intensive care gives the opportunity to critically ill children not only to survive the critical insult but to return in a remarkable quality of life. Given the relative long time needed to achieve this goal, a multidisciplinary approach is guaranteed after discharge to help children, especially in less favorite categories, to achieve their goals. Future research should investigate long-term functional outcome of pediatric intensive care in large multicenter studies.
REFERENCES
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: An updated Pediatric Risk of Mortality score. Crit Care Med 1996; 24: 743–52.
- Tilford JM, Simpson PM, Green JW, et al: Volume-outcome relationships in pediatric intensive care units. Pediatrics 2000; 106:289–94.
- Slater A, Shann F. The suitability of the Pediatric Index of Mortality (PIM), PIM2, the Pediatric Risk of Mortality (PRISM), and PRISM III for monitoring the quality of pediatric intensive care in Australia and New Zealand. Pediatr Crit Care Med 2004; 5:447–54.
- Jones S, Rantell K, Stevens K, et al: Outcome at 6 Months After Admission for PediatricIntensive Care: A Report of a National Study ofPediatric Intensive Care Units in the United Kingdom. Pediatrics 2006; 118:2101-08.
- Edwards JD, Houtrow AJ, Vasilevskis EE, et al: Chronic conditions among children admitted to S. pediatric intensive care units: Their prevalence and impact on risk for mortality and prolonged length of stay. Crit Care Med 2012; 40:2196–2203.
- Butt W, Shann F, Tibballs J, et al: Long-term outcome of children after intensive care. Crit Care Med 1990; 18:961–5.
- Gemke RJ, Bonsel GJ, van Vught AJ. Long-term survival and state of health after paediatric intensive care. Arch Dis Child 1995; 73:196–201.
- Morrison AL, Gillis J, O’Connell AJ, et al: Quality of life of survivors of pediatric intensive care. Pediatr Crit Care Med 2002; 3: 1–5.
- Taylor A, Butt W, Giardulli M. The functional outcome and quality of life after admission to an intensive care unit. Intensive CareMed 2003; 29:795–800.
- Seferian EG, Carson SS, Pohlman A, et al: Comparison of resource utilization and outcome between pediatric and adult intensive care unit patients. Pediatr Crit Care Med 2001; 2: 2–8.
- Volakli EA, Sdougka M, Drossou-Agakidou V, et al: Short-term and long-term mortality following pediatric intensive care. Pediatr Int 2012; 54:248-55.
- Namachivayam P, Shann F, Shekerdemian L, et al: Three decades of pediatric intensive care: Who was admitted, what happened in intensive care, and what happened afterwards. Pediatr Crit Care Med 2010; 11:549-55.
- Conlon NP, Breatnach C, O’Hare BP, et al: Health-related quality of life after prolonged pediatric intensive care unit. Pediatr Crit Care Med 2009; 10:41-44
- Knoester H, Bronner MB, Bos AP. Surviving pediatric intensive care: physical outcome after 3 months. Intensive Care Med 2008; 34:1076-82.
- Ambuehl J, Karrer A, Meer A, et al: Quality of life of survivors of paediatric intensive care. Swiss Med Wkly 2007; 137:312-6.
- Knoester H, Grootenhuis MA, Bos AP. Outcome of paediatric intensive care survivors. Eur J Pediatr 2007; 166:1119–28.
- Butt W. Outcome after pediatric intensive care unit discharge. J Pediatr (Rio J) 2012; 88:1-3.
- Polic B, Mestrovic J, Markic J, et al: Long-term quality of life of patients treated in paediatricintensive care unit. Eur J Pediatr 2013; 172:85-90.
- Fiser DH. Assessing the outcome of pediatric intensive care. J Pediatr 1992; 121: 68–74.
- Fiser DH, Tilford JM, Roberson PK. Relationship of illness severity and length of stay to functional outcomes in the pediatric intensive care unit: a multi-institutional study. Crit Care Med 2000; 28:1173-9.
- Fiser DH, Long N, Roberson PK, et al: Relationship of pediatric overall performance category and pediatric cerebral performance category scores at pediatric intensive care unit discharge with outcome measures collected at hospital discharge and 1- and 6-month follow-up assessments. CritCare Med 2000; 28:2616–20.
- Pollack MM, Holubkov R, Funai T, et al: Relationship between the Functional Status Scale and the Pediatric Overall Performance Category and Pediatric Cerebral Performance Category Scales. JAMA Pediatr. 2014; 168:671-6.
- Alievi P, Carvalho PRA, Trotta EA, et al: The impact of admission to a pediatric intensive care unit assessed by means of global and cognitive performance scales. J Pediatr (Rio J) 2007; 83:505-11.
- Volakli E, Sdougka M, Tamiolaki M, et al: Demographic profile and outcome analysis of pediatric intensive care patients. Hippokratia 2011; 15:316-322
- Anderson V, Godfrey C, Rosenfeld VJ, et al: Predictors of cognitive function and recovery 10 years after traumatic brain injury in young children. Pediatrics 2012; 129:e254– e261.
- Gabbe BJ, Simpson PM, Sutherland AM, et al: Functional and health-related quality of life outcomes after pediatric trauma. J Trauma 2011; 70: 1532-8.
Author Disclosures: Authors Volakli E, Sdougka M, Mantzafleri PE, Tsonidis Ch, Kontopoulos E, Tsikoulas I have no conflicts of interest or financial ties to disclose.
Corresponding author:
Eleni A. Volakli,
Xylouri 26, 56626,
Thessaloniki, Greece
E-mail:






