
Authors: Mouloudi E. MD, PhD, Papadopoulos S., MD, Massa E. MD, Giasnetsova T. MD, Theodoridou Th. MD,Anastasiou A. MD, PhD, Fouzas I. MD, PhD, TsonidisCh. MD, PhD, PapanikolaouV. MD, PhD, Gritsi-Gerogianni N. MD, PhD
ABSTRACT
Neurologic complications after liver transplantation are quite common, with central pontine myelinolysis (CPM) being a rare but fatal complication. In this report, we describe the case of female liver transplant recipient who developed CPM after orthotopic liver transplantation (OLT).A 62-year old woman was admitted to the ICU for postoperative recovery after OLT. The procedure was described as uneventful. The patient had a history of decompensated cirrhosis, tension ascites, class I hepatic encephalopathy and chronic hyponatremia which necessitated repeated hospitalizations in the year prior to transplantation.The patient was unable to be weaned from ventilator support and did not show an improvement in mental status (GCS=5) despite the cessation of sedation. After neurologic consultation, a brain MRI was performed which showed evidence of CPM in the pons. Despite supportive therapy, the patient did not show an improvement of mental status and after a 55-day hospitalization in the ICU she died from septic complications.The etiology of CPM is multifactorial, with liver transplant recipients being at an increased risk. Supportive treatment is the standard of care, and there are not enough evidence supporting other types of treatment.
INTRODUCTION
Neurologic complications after liver transplantation are quite common, ranging from 15-30% of liver transplant recipients, usually attributable to immunosuppressant neurotoxicity and opportunistic infections1. Central pontine myelinolysis (CPM) is a concentrated noninflammatorydemyelination in the central basis pontis and in 10% of cases there are extrapontine sites of myelinolysis detected (midbrain, basal nuclei, thalamus and cerebellum). It was first described by Adams et al in 1958 in cases of alcoholic and/or malnourished patients2. Typically it shows a biphasic clinical course, initially with encephalopathy or hyponatremic seizures, then recovery as sodium levels are corrected, to deterioration several days later to dysphagia/dysarthria, quadriparesis, locked-in syndrome and coma3. Risk factors include severe hyponatremia (<120mEq/l for more than 48 hrs), aggressive serum sodium correction and development of hypernatremia during tratment. Initially the outcome was bleak, but with later advents in imaging, MRI availability and new concepts in electrolyte management mortality rates have dropped, but still remain significant and with variable neurologic sequelae which require extensive and prolonged rehabilitation.4
Case description
a. History
The patient was a 62-year old woman who was admitted to our ICU for postoperative care after orthotopic liver transplantation for decompensated cirrhosis due to autoimmune hepatitis. Her past medical history included diabetes mellitus and osteoporosis with vertebral compression fractures. She was treated repeatedly for chronic hyponatremia (in the range of 119-128 mEq/L), tension ascites (repeated transdermal drainages) and mental status alterations (last episode 1 month prior to transplantation). The patient was hospitalized for 1 month prior to transplantation to an internal medicine ward (due to mental status alteration, tension ascites and hyponatremia) where she underwent a brain CT scan without any significant findings. The preoperative MELD score was 23.
b. Clinical course
The patient underwent an orthotopic liver transplantation from a cadaveric donor without any significant intraoperative events and with an operative time of 6.5 hours. Intraoperative transfusion requirements were: 8 units of packed red cells, 21 units of fresh frozen plasma and 19 units of platelets. She was transferred immediately postoperatively in the ICU for recovery. From the 1st postoperative day she was put on methylprednisolone (and mycophenolate mofetil from the 3rd postoperative day) for immunosuppression. No graft dysfunction or rejection was evident in her entire postoperative course.
The first weaning attempt was performed on the 3rd postoperative day, without any significant neurological finding up to that time (the patient was sedated with propofol and remifentanyl). The patient showed a Glasgow Coma Scale of 5 (E2M2V1) without sedation, with only slight reactions to painful stimuli. Serum ammonia levels were not markedly increased (24-28 μmol/l). After neurologic consultation, a brain CT scan was performed, which showed no significant findings apart from mild leucoencephalopathy. Because of the patient’s neurologic history and her present condition, an early percutaneous tracheostomy (6th postoperative day) was performed to facilitate weaning from ventilatory support. The patient from then on showed a steady improvement, but her neurologic status remained unchanged, with a GCS of 5-6 and slight reactions only to painful stimuli. On the 13th postoperative day a brain MRI scan showed an abnormal MR signal in the pons (figure 1).
After neurologic and radiological consultations, this finding was verified as a focus of pontine myelinolysis, which was not found to be related to any electrolyte management perioperatively.
c. Outcome
The patient never showed an improvement in her neurologic status and repeatedly failed spontaneous breathing (t-piece) trials, necessitating a 55-day length of stay in the ICU on almost continuous ventilatory support, with concomitant episodes of carbapenemase-resistant Klebsiella pneumoniae infection. She died from severe multiorgan failure due to sepsis on the 55th postoperative day.
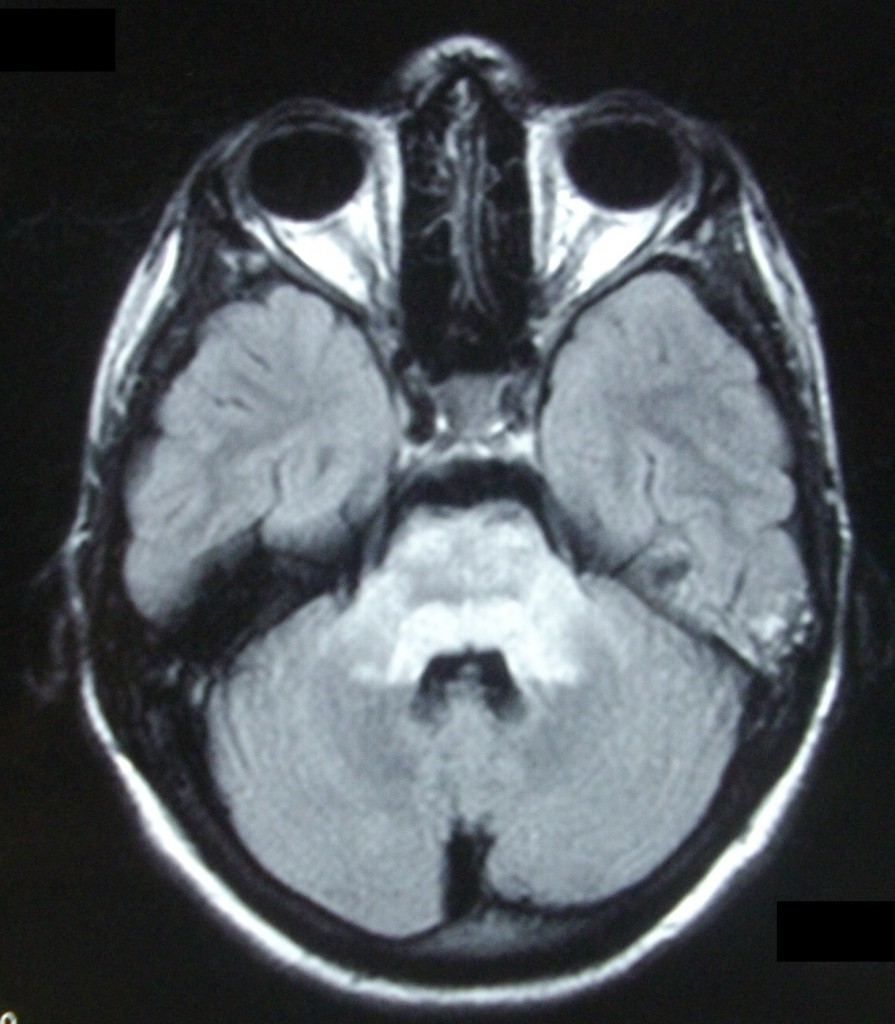
Figure 1: The patient’s brain MRI scan during ICU stay, showing a “bright” area in the pons on T2-wighted sequence, indicative of CPM.
Discussion
Central pontine myelinolysis is a rare (recorded as 0.88% in one study5) but potentially fatal complication in liver transplant recipients. A high MELD score and a preoperative hyponatremia are important risk factors5, as in our patient. The rapidity of serum sodium correction is not the only culprit, with immunosuppressant toxicity, alcoholism, malnutrition and liver transplantation being additional factors for the development of myelinolysis. There is an ongoing debate about how aggressive or conservative sodium correction should be, rendering the process more empiric3.
In our case, immunosuppressant toxicity was ruled out due to the patient’s history and sodium correction before and after transplantation was not markedly aggressive. In many cases diagnosis is difficult and achieved mainly by exclusion. Supportive treatment is the standard of care, and there are not enough evidence supporting other types of treatment1.
REFERENCES
- Zivković SA. Neurologic complications after liver transplantation.World J Hepatol. 2013 Aug 27;5:409-16.
- Adams RA, Victor M, Mancall EL. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholics and malnourished patients. Arch Neurol Psychiatry 1959;81:154–72.
- Martin RJ. Central pontine and extrapontine Myelinolysis: the osmotic Demyelination syndromes. J Neurol Neurosurg Psychiatry 2004;75(Suppl III):iii22–iii28.
- Luzzio C. Central Pontine Myelinolysis. Medcape.http://emedicine.medscape.com/article/1174329-overview
- Lee EM, Kang JK, Yun SC, et al.Risk factors for central pontine and extrapontine myelinolysis following orthotopic liver transplantation.Eur Neurol. 2009;62:362-8.
Author Disclosures: Authors MouloudiE, Papadopoulos S, MassaE, GiasnetsovaT, TheodoridouTh, AnastasiouA, FouzasI, TsonidisCh, PapanikolaouV, Gritsi-GerogianniN have no conflicts of interest or financial ties to disclose.
Corresponding author:
Eleni Mouloudi
85 Mantineas Street, 54248,
Thessaloniki,Greece.
E-mail:






