
Authors: Massa E MD, MSc, Mouloudi E MD, PhD, Kydona Ch MD, Papadopoulos S MD, Sgourou K MD, Gritsi-Gerogianni N MD, PhD.
Intensive Care Unit, Hippokration University Hospital, Thessaloniki Greece
ABSTRACT
We report a rare case of a young woman with anti-N-Methyl-D-Aspartate receptor (NMDAR) encephalitis, who developed psychiatric symptoms, dyskinesias, hypoventilation, hypersalivation and seizures. Serial analysis of antibodies to NR1/NR2B heteromers of the NMDAR was positive on the patient’s serum and cerebrospinal fluid (CSF). Removal of an ovarian teratoma after intravenous immunoglobulin and corticosteroid therapy resulted in a prompt neurological response.
INTRODUCTION
Since its discovery in 2007, the encephalitis associated with antibodies against N-Methyl-D-Aspartate Receptor (NMDAR) has entered the mainstream of neurology and other disciplines.
Paraneoplastic limbic encephalitis (PLE) is a rare neurological syndrome characterized by short-term memory impairment, seizures, involuntary movements and various psychiatric disturbances. It is often associated with breast cancer, germ-cell testicular tumors and small cell lung cancer, but rarely with ovarian teratomas2. PLE associated with ovarian teratoma has recently been related to the development of antibodies to the NR1/NR2B heteromers of the N-Methyl-D-Aspartate Receptor (NMDAR), the disorder being named anti-NMDAR encephalitis2.
Despite the severity of symptoms, most patients recover if the disorder is recognized and treated in time. Immumotherapy is often effective and it has been suggested that prompt resection of the teratoma expedites recovery2.
In most previously reported cases of NMDAR encephalitis, the ovarian teratoma was removed a few months (median: 9 weeks) after the presentation of neurological symptoms, sometimes when symptoms had already partially responded to immunotherapy2-6.
We report the outcome in a young woman whose ovarian teratoma was removed one month after the onset of neurological symptoms.
CASE REPORT
A 38 year old woman with a free medical history presented to a rural hospital complaining of headache, progressively worsening dizziness, fever with concomitant tremors, confusion, disorientation, short term memory loss and upper limb tremors.
She was initially admitted with the diagnosis of viral encephalitis and treated with acyclovir, mannitol and phenytoin. After 4 days of hospitalization her condition worsened (symptom persistence, mental status deterioration) and she was intubated and transferred to the Intensive Care Unit (ICU) of a tertiary hospital (ours). On admission the patient showed mild fever and was hemodynamically stable. Cerebrospinal fluid (CSF) examination showed a clear, colorless CSF with high protein (60 mg/dl) and glucose content (110mg/dl). CSF cytology (Table 1)was negative for Herpes simplex 1 & 2 viruses (HSV 1 & 2), cytomegalovirus (CMV), Epstein-Barr virus (EBV), varicella-zoster virus (VZV), measles, rubella, H1N1 influenza virus and leishmania. Antibodies were also negative for toxoplasmosis, rickets, Lyme disease, West Nile fever and syphilis. Serologic examination (table 2) for antinuclear antibodies, P & C-ANCA complement, immunoglobulins, tumor markers and paraneoplastic antibodies (including anti-H4, Yo-R1, amphiphysin) was negative in the CSF and serum. Serologic testing for thrombopilia was also negative (Table 1).
Table 1. Patient Serology
| Serum | Cerebrospinal Fluid | Bronchial secretions | Serum | ||
|---|---|---|---|---|---|
| Viral and other infectious agents | |||||
| HSV 1-2 | Negative | Negative | NK lymphocytes | ||
| CMV | Negative | CD3+/CD1656+ | 0.05% | ||
| B. burgdorferi | Negative | CD3/CD 1656+ | 0,76 % (6,23) | ||
| Rubella | Negative | B-lymphocytes | |||
| Measles | Negative | CD 20+ | 20.00% | ||
| Η1Ν1 | Negative | Helper/cytotoxic ratio | inverted | ||
| Epstein-Barr | Negative | Tumor markers | negative | ||
| Leishmania | Negative | Erythrocyte sedimentation rate (mm/h) | 20 -80 | ||
| Adenovirus | Negative | C-reactive protein | 6,04-115 | ||
| Cosxsackiae | Negative | Hormone screening | |||
| Echo | Negative | Thyroid hormones | normal | ||
| Parvo | Negative | Follicle Stimulating hormone (FSH) | 2,64 | ||
| Legionella | Negative | Luteinizing Hormone (LH) | 0,18 | ||
| Rickettsia conori | Negative | Estradiol | 64,9 | ||
| Rickettsia mooseri | Negative | ||||
| Syphilis | Negative | ||||
| Immunologic markers | Immunoglobulins | ||||
| ΑΝΑ | Negative | IgA | 130 (normal) | ||
| C3 | 3,2 | IgG | 420 | ||
| CAMA | 10 | IgM | 71 (normal) | ||
| MPO | 3,1 | ||||
| Ra-test | <20,0 | ||||
| T-lymphocytes | |||||
| CD3+ | 59,10% | ||||
| CD4+ | 20,10% | ||||
| CD3+/CD8 | 50,60% | ||||
| CD4+/CD8+ ratio | 0,4 |
Table 2. Patient immunologic markers
| Lupus antigoagulant (LA): Negative | T-lymphocytes |
|---|---|
| CD3+ : 59,1% | |
| CD4+: 20,1 % | |
| CD3+/CD8: 50,6 % | |
| CD4+/CD8+ ratio : 0,4 | |
| NK lymphocytes | |
| Immunoglobulins | CD3+/CD1656+ : 0,05 % |
| IgA: 130 (normal) | CD3/CD 1656+ : 0,76 % (6,23) |
| IgG: 420 | B-lymphocytes |
| IgM: 71 (normal) | CD 20+ : 20% |
| Cellular immunity disturbances | |
| T-lymphocyte series defect | |
Computed Tomogrpahy (CT) and Magnetic Resonance Imaging (MRI) scans (Figure 1) of the brain showed a mildly increased MR signal in the hippocampic region in T2 and FLAIR sequences without abnormal enrichment after intravenous contrast medium administration, a picture compatible with limbic encephalitis. Abdominal CT scanning and sonography showed a mature cystic teratoma in the right ovary, about 5 centimeters in diameter.
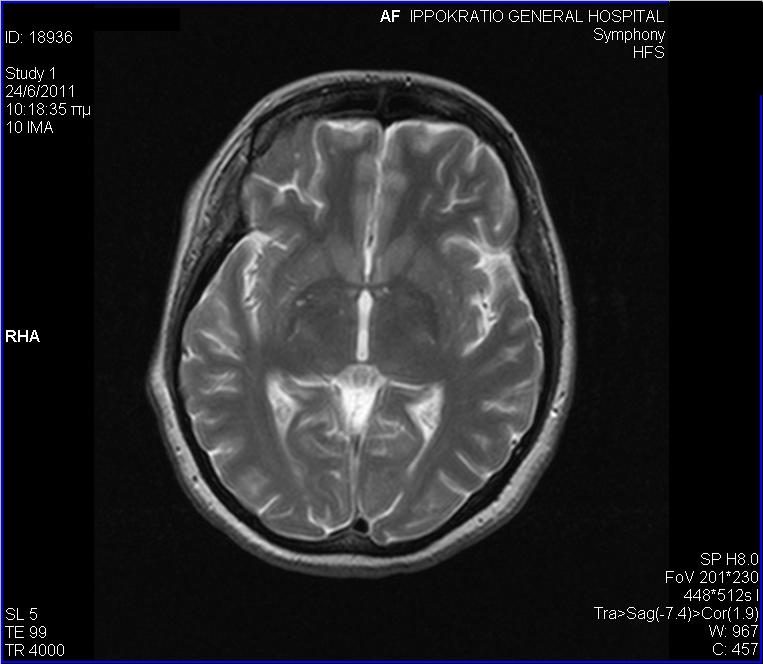
Figure1. Cerebral Magnetic Resonance Imaging (MRI): Slightly increased MR signal in T2-FLAIR images in the hippocampus, without abnormal enrichment after i.v. administration of contrast agent. These finding were suggestive of limbic encephaliltis.
Initial therapy included acyclovir 2250mg/day, dexamethasone 32 mg/day and phenytoin. The patient’s clinical condition deteriorated with the presentation of sucking motion of the mouth, labial, lingual and ocular dyskinesias, salivation and loss of consciousness. Antiepileptic treatment was increased, including sodium valproate, clonazepam, levetiracetam, lacosamide and from time to time intravenous midazolam. Electroencephalography (EEG) showed continuous and arrhythmic delta waves in both hemispheres. Techetium-99-HMPA brain scintigraphy (Figure 2) showed findings compatible with, but not specific to diffuse microangiopathy.

Figure 2. Single-photon emission computed tomography with TC99m-HMPAO: Marked decrease in scintigraphic agent uptake in the parietal lobes bilaterally. A smaller decrease is observex in the left occipital and lower left temporal lobe and in the medial frontal and prefrontal lobes bilaterally. These findings are compatible with diffuse microangiopathy but not specific to the condition.
The clinical and imaging findings of limbic encephalitis on one hand and the ovarian teratoma on the other narrowed the differential diagnosis to paraneoplastic or autoimmune encephalitis, which was confirmed by a positive test for anti-neuronal antibodies(Table 3).
Table 2. Patient immunologic markers
| Lupus antigoagulant (LA): Negative | T-lymphocytes |
|---|---|
| CD3+ : 59,1% | |
| CD4+: 20,1 % | |
| CD3+/CD8: 50,6 % | |
| CD4+/CD8+ ratio : 0,4 | |
| NK lymphocytes | |
| Immunoglobulins | CD3+/CD1656+ : 0,05 % |
| IgA: 130 (normal) | CD3/CD 1656+ : 0,76 % (6,23) |
| IgG: 420 | B-lymphocytes |
| IgM: 71 (normal) | CD 20+ : 20% |
| Cellular immunity disturbances | |
| T-lymphocyte series defect | |
In the immediate postoperative period the dyskinesias subsided significantly and were totally absent for 10 days, to reappear later on.
On the 17th day of hospitalization the patient underwent a percutaneous tracheostomy, due to her impaired neurologic status and inability to wean her from mechanical ventilation. During her hospitalization she presented multiple episodes of sepsis. She was weaned from ventilatory support and was discharged from the ICU after 3 months, with no consciousness, with spontaneous eye opening, labial and lingual dyskinesias and upper and lower extremity tremors bilaterally.
Discussion
We determined that this patient had definite paraneoplastic encephalitis, with predominant involvement of the limbic system. Accordingly, she developed a gradual loss of short-term memory, seizures, psychiatric symptoms, MRI abnormalities in the limbic system and positive titres for antineuronal antibodies6-8.
Central nervous system tissue in the teratoma might be a trigger of the immune reaction. The majority of teratomas are mature cystic ones. Immature teratomas (constituting 1% of all teratomas) were present in 29% of anti-NMDAR related cases9. Bilateral teratomas were present in 14% of cases, comparable to 12% described in general.
Development of paraneoplastic syndromes in the setting of gynecologic malignancy is rare. When they occur, the neurologic symptoms most often precede and usually lead to the diagnosis of malignancy. Early diagnosis and aggressive treatment of the underlying tumor may stabilize or improve the neurologic abnormalities. Paraneoplastic neurological syndromes (PLE) have been treated with intravenous immunoglobulin and/or corticosteroids with plasmapheresis, with varying results.
The majority of patients with PLE and teratoma improved after tumor resection10,11,12. In our case, the ovarian teratoma was diagnosed 10 days after the onset of psychiatric symptoms, and was removed 30 days after, while the patient received immunoglobulin and corticosteroid therapy.
We believe that prompt tumor resection is the most important factor for immediate improvement and possible cure of NMDAR encephalitis.
Prompt treatment may decrease the duration of mechanical ventilatory support and the frequency of dyskinesias in comparison with patients where the tumor was not removed13.
After reviewing the literature1, it was noted that the involuntary facial movements and dyskinesias are usually very resistant to therapy, as it was in our case. In our patient, a teratoma was also found on the left ovary, and a partial ovarian resection and tumor resection was performed, a fact which could explain the shot-term regression of the dyskinesias and their reappearance along with the poor neurological progression of the patient.
According to the literature14, in a study published in the Lancet in 2008 and regarded 100 cases with NMDAR-antibody positive encephalitis, the majority of patients were women (91%) with an average age of 23 years old. A malignancy was present in 58% of the patients, with ovarian teratoma the most frequent. All patients showed psychiatric symptoms and loss of short-term memory. Seventy-six percent of patients had full loss of consciousness, 86% showed dyskinesias, 76% tremors, 69% autonomic nervous system instability, and 66% presented hypoventilation.
Patient prognosis was good or with minimal residual neurologic defects in 75% of cases, while 25% of patients had serious neurologic impairment or expired. The patients who improved showed a reduction in anti-neuronal antibody titres
REFERENCES
- Gultekin S H, Rosenfeld MR, Voltz R. et al Paraneoplastic limbic encephalitis: neurological symptoms, immunological findings and tumour association in 50 patients. Brain 2000;123:1481–94.
- Dalmau J, Tüzün E, Wu HY, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007;61:25–36.
- Iizuka T, Sakai F, Ide T, et al. Anti-NMDA receptor encephalitis in Japan: Long-term outcome without tumor removal. Neurology 2008; 12; 504-11.
- Koide R, Shimizu T, Koike K, et al. EFA6A-like antibodies in paraneoplastic encephalitis associated with immature ovarian teratoma: a case report. J Neurooncol. 2007;81:71–4.
- Shimazaki H, Ando Y, Nakano I, et al. Reversible limbic encephalitis with antibodies against the membranes of neurons of the hippocampus. J Neurol Neurosurg Psychiatry. 2007;78: 324–5.
- Tonomura Y, Kataoka H, Hara Y, et al. Clinical analysis of paraneoplastic encephalitis associated with ovarian teratoma. J Neurooncol. 2007;84: 287–92.
- Baumgartner A, Rauer S, Mader I, et al. Cerebral FDG-PET and MRI findings in autoimmune limbic encephalitis: correlation with autoantibody types. J Neurol. 2013;260:2744–53.
- Finke C, Kopp UA, Pajkert A, et al. Structural Hippocampal damage following anti-N-methyl-D-aspartate receptor encephalitis. Biol Psychiatry. 2016;79(9):727–34.
- Graus F, Delattre J Y, Antoine J C. et al. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry 2004. 751135–1140.
- Titulaer M.Soffietti, Dalmau J, et al. Screening for tumours in paraneoplastic syndromes : report of an EFNS Task Force.Eur J.Neurol. 2011;18:19-e3
- Vitaliani R, Mason W, Ances B, et al. Paraneoplastic encephalitis, psychiatric symptoms, and hypoventilation in ovarian teratoma. Ann Neurol 2005;58:594–604.
- Harald H, ChristianU, Astrid G, et al. Bi-insular cortical involvement in anti-NMDA-receptor encephalitis – a case report. BMC Neurology 2016; 16: 130.
- Shimazaki H, Ando Y, Nakano I, et al. Reversible limbic encephalitis with antibodies against the membranes of neurones of the hippocampus. J Neurol Neurosurg Psychiatry. 2007; 78: 324–5.
- Iizuka T, Sakai F, Ide T, et al. Anti-NMDA receptor encephalitis in Japan: Long-term outcome without tumor removal. 2008 Feb 12;70:504-11
Author Disclosures:
Authors Massa E., Mouloudi E., Kydona Ch., Papadopoulos S., Sgourou K., Gritsi-Gerogianni N. have no conflicts of interest or financial ties to disclose.
Corresponding author:
Μassa Eleni MD MSc,
Hippokratio University Hospital,
Konstantinoupoleos 49 Thessaloniki, Greece
e-mail: Tel:2310892357, 6944441323






