
Authors: Vrigga M MD, Papagiannopoulou P MD, PhD, Ntritsou V MD, PhD, Isaakidis A MD, Chatziiokimidis Ch MD, Kostoglou Ch MD, Zachariadou Ch MD
ABSTRACT
The aim of this study was to compare the combination of oral tramadol and midazolam to oral midazolam alone, in children undergoing adenotonsillectomy, as an oral premedication, regarding also sedation and postoperative pain relief. Sixty children selected for elective adenotonsillectomy were enrolled in this randomized, controlled prospective study. Patients were randomly allocated into two groups. Group M (n=30) received 0.5 mg.kg-1 oral midazolam and group MT (n=30) received 0.2 mg.kg-1 oral midazolam with 1 mg.kg-1 oral tramadol as a premedication 30min preoperatively. Standard general anesthesia technique was used. A 5 points-sedation score (1 asleep to 5 agitated) on arrival to the operating room, a 3 points-acceptance score of separation from the parents and a 3 points-mask cooperation score at induction of anesthesia (1 easy to 3 markedly resistant) were used. Aldrete score, extubation time and intraoperatively consumption of remifentanil were also recorded. Pain intensity was assessed using a modification of the Hannallah pain score scale at 30min, 6h and 24h postoperatively. If pain score was higher than 3, additional analgesics were provided. Cumulative analgesic consumption in 24hrs was also noted. A satisfactory level of sedation scores were recorded in both groups. Group MT offered significantly more children in an awake, calm and quiet state, who were easily separated from their parents. The parental separation scores did not differ statistically significant between groups. The mask acceptance was statistically significant easier in group MT, while children in midazolam group (group M) were statistically significant resistant compared to children in group MT. Pain and modified Aldrete scores were comparable between groups. The amount of remifentanil consumed intraoperatively was statistically significant lower in group MT. Postoperative analgesic consumption was lower in group MT compared to group M but with no statistical significance. Adding oral tramadol to midazolam as a premedication in children provides good quality of sedation and decreases perioperative analgesic requirements following adenotonsillectomy.
INTRODUCTION
The preoperative period is usually a stressful time for children and their parents1. Uncooperative children, whether due to anxiety, phsychologic, developmental or mental disorders or repeated anesthesia, should be adequately treated in order to avoid postoperative behavior problems2,3. Various interventions are used to allay the anxiety of a child during the perioperative period such as sedative premedications, parental presence during induction and preoperative preparation programs4,5. Sedation remains one of the widely used methods for decreasing anxiety in young children. The oral route remains the most acceptable method of drug administration though various combinations of drugs and routes of administration are available6.
Adenotonsillectomy is a common pediatric surgical procedure associated with significant postoperative pain7. Inadequate pain management after this procedure is a difficult task and could remain even over four days after surgery and results in poor oral intake, dehydration, long hospital stay, sleeping disorders, behavioral changes, nausea and vomiting8.
Various methods and medications are available to relieve and control preoperative stress and acute postoperative pain in children after adenotonsillectomy. Midazolam with its favorable pharmacodynamics (i.e. rapid onset, relatively short duration and lack of significant side effects)6,7, and pharmacokinetics is among the most popular pediatric premedicant in Europe and U.S.A7. However good to excellent results are seen in only 60-80% of cases9.
Suitable doses of the major analgesics are routine for in-patient children’s surgery. However, fear of side effects such as nausea and vomiting or respiratory depression prevents the wide use of powerful opioids in children10. Tramadol hydrochloride is a synthetic analogue of codeine used for the treatment of moderate to severe pain. It has a dual mechanism of action. Tramadol and its active metabolite, O-desmethyl tramadol, bind to μ opioid receptors thus exerting their effect on GABAergic transmission. They also inhibit reuptake of 5-hydroxy tryptamine (serotonin) and noradrenaline11. These latter effects are likely to be an important element in analgesia and may also account for triggering two significant adverse events – seizures and serotonin syndrome12. These may develop during tramadol monotherapy either at routine or excessive doses, but are particularly likely during tramadol administration in epileptic patients13.
Tramadol has been licensed for use in children over 1 year of age in many European countries, although others have limited its use to children over 12 years of age14. Pharmacokinetic data is available in young children following intravenous and caudal routes of administration, but few kinetic studies have been published using oral drop administration in children14.
Midazolam and tramadol can be used in different dosage combinations with variable effects and outcomes. A combination with lower doses of them could provide adequate anxiolysis, sedation and postoperative pain relief with lesser fewer side effects15. Therefore, the authors thought that a combination of midazolam with tramadol may be useful to enhanced preoperative stress and postoperative pain relief after adenotonsillectomy. Thus, the goal was to study the combination of oral tramadol and midazolam to oral midazolam alone, in children undergoing adenotonsillectomy, as an oral premedication, regarding also sedation and postoperative pain relief.
MATERIAL AND METHODS
Following institutional approval and written informed parental consent, which abided with the Declaration of Helsinki, 60 children, 3-12 years of age with ASA physical status I or II, scheduled for elective adenotonsillectomy, as in-patients, were recruited in this prospective randomized double blinded study. All operations were performed by the same surgeon who was blind to the study drug, using the same surgical technique.
Exclusion criteria included children with ASA physical status III or higher, neurological and cardiovascular system disorders, history of seizures or epilepsy, increased intracranial pressure, upper respiratory tract infection and documented allergies. Patients who developed bleeding or hypersensitivity to tramadol and those who refused to swallow or vomited the premedication mixture also were excluded from the study.
All children were randomly assigned in two groups, using computer-generated random numbers. Group M (n=30) received 0.5 mg.Kg-1 oral midazolam and group MT (n=30) low dose combination of oral midazolam (0.2 mg.kg-1) and tramadol drops (1 mg.kg-1). Both medications were mixed in 5 ml apple juice by a nurse not involved in the study and administrated to the patients 30 minutes prior to anesthesia induction.
On arrival at the operating room children were evaluated with a scoring system for premedication assessment, which consisted of a 5 points-sedation score (1 asleep to 5 agitated), a 3 points-acceptance score of separation from the parents and a 3 points-mask cooperation score at anesthesia induction (1 easy to 3 markedly resistant)16 (Table 1).
Table 1.The scoring system for premedication assessment in children
| Five points-sedation score | |
| Agitated | 1 |
| Restless | 2 |
| Calm, but awake | 3 |
| Asleep, but arousable | 4 |
| Asleep, not readily arousable | 5 |
| Score for separation acceptance from parents | |
| Easy | 1 |
| Slightly resistant | 2 |
| Markedly resistant | 3 |
| Mask acceptance score | |
| Easy | 1 |
| Slightly resistant | 2 |
| Markedly resistant | 3 |
Scores 2 and 3 in the sedation score were defined as ‘effective’ and score 3 for separation from the parents and mask cooperation at anesthesia induction was defined as ‘poor’.
All study patients received a standard anesthetic protocol. Anesthesia was induced with sevoflurane in 100% oxygen administrated via mask and breathing circuit. Monitoring consisted electrocardiogram, pulse oximetry, automated non-invasive blood pressure, end-tidal carbon-dioxide, inhalation agent concentration and an FiO2 (fraction of inspired oxygen) analyser. After obtaining intravenous (i.v) access, fentanyl (3 mcg /kg), lidocaine (1 mg/kg) and rocuronium (0.6 mg/kg) were administrated, followed by tracheal intubation using an appropriate-sized endotracheal tube. Anesthesia was maintained with sevoflurane in oxygen 40% titrated to clinical response. Intermitted positive pressure ventilation was used. Intraoperative analgesia was provided with remifentanil i.v infusions of 0.05 to 1 mcg/kg/min, with bolus doses of 1 mcg/kg if needed, in order to maintain heart rate and systolic blood pressure within 20% of the baseline levels. Intraoperative consumption of remifentanil was noted during the study. At the end of surgery, residual neuromuscular blockade was reversed with neostigmine (50 mcg/kg) and atropine (20 mcg/kg). After adequate neuromuscular recovery and return of airway reflexes, the trachea was extubated.
The duration of surgical procedure and anesthesia and the time interval between discontinuation of anesthesia and arousal (spontaneous ventilation, extubation) were recorded. Postanesthetic recovery was also assessed, where as heart rate, blood pressure, respiratory rate and pulse oximetry were noted, until the child was fit for discharge using the modified Aldrete criteria7,17 (Table 2). A modified Aldrete score nine 9 or more was required for recovery of the patient to be confirmed.
Pain intensity was assessed using a modification of the pain score scale originally described by Hannallah et al., at 30 min, 6h and 24h postoperatively, by a blind observer7,18. This pain score scale allowed for a maximum score of 10 and a minimum of 0. The modification was to allow observation and scoring of pain on swallowing water as opposed to pain on movement (Table 3).
Additional analgesia was provided when pain scores were higher than 3. Pain was treated with rectally use of paracetamol (20 mg/kg) and cumulative paracetamol consumption in 24 hours was used to compare postoperative analgesic requirements in both study groups. Side effects related to the administered drugs, such as postoperative nausea, vomiting, apnea or airway obstruction were also noted.
Table 2. Modified Aldrete scoring system*
| Activity: able to move, voluntarily or on command | |
| Four extremities | 2 |
| Two extremities | 1 |
| No extremities | 0 |
| Respiration | |
| Able to breathe deeply and cough freely | 2 |
| Dyspnea, shallow or limited breathing | 1 |
| Apnoea | 0 |
| Circulation | |
| Blood pressure within 20mmHg of preoperative level | 2 |
| Blood pressure within 20-50mmHg of preoperative level | 1 |
| Blood pressure ±50mmHg of preoperative level | 0 |
| Circulation | |
| Blood pressure within 20mmHg of preoperative level | 2 |
| Blood pressure within 20-50mmHg of preoperative level | 1 |
| Blood pressure ±50mmHg of preoperative level | 0 |
| Consciousness | |
| Fully awake | 2 |
| Arousable on calling | 1 |
| Unresponsive | 0 |
| Oxygen saturation | |
| Saturation >92% | 2 |
| Needs oxygen to maintain saturation >90% | 1 |
| Saturation <90% with oxygen | 0 |
Table 3. Pain scoring system.
| Crying | |
| Non | 0 |
| Consolable | 1 |
| Inconsolable | 2 |
| Movement | |
| Non | 0 |
| Restless | 1 |
| Thrashing | 2 |
| Agitation | |
| Sleep or calm | 0 |
| Mild | 1 |
| Hysterical | 2 |
| Swallowing secretions | |
| Normal | 0 |
| Uncomfortable | 1 |
| Unable | 2 |
| Complaints of pain | |
| Asleep or non | 0 |
| Cannot localize | 1 |
| Localizes | 2 |
Data were expressed as the mean ± SD analyzed using tests of significance to identify the variables significantly to differences in different groups. Student t-test and Chi square test were used. Statistical significance was assumed, at level of p<0.05. Analysis was performed with the Statistical Package for the Social Sciences (SPSS, Inc., Chicago IL).
RESULTS
There was no statistically significant difference, between groups, regarding demographic data, duration of surgery and duration of anesthesia procedure (Table 4). All children accepted the premedication mixture well and no incidence of vomiting or refusal to swallow was noted. A total of 60 children (n=30 in each group) were included in this study.
Hemodynamic parameters remained within 20% of the baseline values throughout the study and no statistical significant differences between groups were recorded. Children in group MT exhibited a significantly lower time interval between discontinuation of anesthesia, spontaneous ventilation and extubation compared to the corresponding in group M (Table 4).
Table 4. Perioperative data.
| Group M (n=30) | Group MT (n=30) | p | |
| Age (years) | 5.73±2.34 | 5.53±2.01 | NS |
| Weight (Kg) | 23.5±9.24 | 24.63±9.98 | NS |
| Gender (f/m) | 14/16 | 12/18 | NS |
| ASA (I/II) | 29/1 | 28/2 | NS |
| Duration of anesthesia (min) | 64.1±19.26 | 62.43±18.98 | NS |
| Duration of surgery (min) | 41.57±17.97 | 46.57±16.48 | NS |
| Time to extubation (min) | 22.53±8.39 | 17.2±9.53 | p<0.05 |
| Remifentanil consumption (mcg) | 134.3±109.2 | 112.1±67.8 | p<0.05 |
| Modified Aldrete score | 9.03±0.6 | 9.2±0.58 | NS |
On arrival to the operation room one patient (3.33%) in group M was asleep but not arousable, while none of the patients in group MT were in such state, with no statistical significance between groups. Specifically in group M 86.6% of children presented effective sedation (sedation score 2 or 3), and 96.6% of patients in group MT. In group M, patients with sedation score 2 (sleep, but arousable) were statistical significantly fewer compared with the corresponding in group MT (p<0.05) (Table 5).
There were no statistical significant differences between groups concerning parental separation. Three patients in group M showed poor separation score (separation score 3) compared with one patient in group MT (Table 5).
Regarding mask cooperation scores, 16 (53.3%) patients in group M showed statistical significantly less easy mask acceptance compared to 26 (86.6%) patients in group MT (p<0.05). “Slightly resistant” to mask were statistical significant more patients in group M (33.3%) than in group MT (6.66%) (p<0.05). Only two patients in group MT presented “poor mask cooperation” compared to four patients in group M, with no statistical significance (Table 5).
The amount of remifentanil administered intraoperatively was statistical significant lower in group MT compared to group M (p<0.05) (Table 4).
Table 5. Sedation score, parental separation score and mask cooperation score.
| Group M No pts (%) | Group MT No pts (%) | p | |
| Sedation score | |||
| 1 | 1 (3.33%) | 0 (0%) | NS |
| 2 | 3 (10%) | 9 (30%) | p<0.05 |
| 3 | 23 (76.6%) | 20 (66.6%) | NS |
| 4&5 | 3 (10%) | 1 (3.33%) | NS |
| Parental separation score | |||
| 1 | 24 (80%) | 26 (86.6%) | NS |
| 2 | 3 (10%) | 3 (10%) | NS |
| 3 | 3 (10%) | 1 (3.33%) | NS |
| Mask cooperation score | |||
| 1 | 16 (53.3%) | 26 (86.6%) | p<0.05 |
| 2 | 10 (33.3%) | 2 (6.66%) | p<0.05 |
| 3 | 4 (13.3%) | 2 (6.66%) | NS |
Recovery from anesthesia was assessed using a modified Aldrete score, which was comparable between groups (Table 4).
Concerning pain intensity, at the end of adenotonsillectomy (30min), 6h and 24h following surgery, groups M and MT did not differ statistically significant. Even though patients, who received midazolam (Group M) reported higher pain scores at all times intervals (Figure 1).

Figure 1. Pain scale, during the first 24 h after adenotonsillectomy in the two groups. M group premedicated with midazolam and MT group premedicated with midazolam plus tramadol.
Midazolam group (Group M) received higher doses of rectal paracetamol compared to midazolam plus tramadol group (Group MT), but with no level of significance (Figure 2).
In addition, there were no episodes of apnea or airway obstruction noted, after premedication or in the postoperative period, in both study groups. Only one child in group MT experienced vomiting, but it was self limited and did not require any pharmacological intervention.
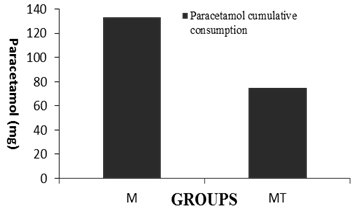
Figure 2. Consumption of analgesics (supp. Paracetamol) during the first 24 h after operation in the two groups. M group premedicated with midazolam and MT group premedicated with midazolam plus tramadol.
DISCUSSION
This study shows that both midazolam and the combination of midazolam-tramadol, when used in children undergoing adenotonsillectomy, as an oral premedication, are satisfactory in terms of acceptable sedation, acceptability to the patient and concerning the incidence of postoperative complications. The results, also, showed that the combination of oral midazolam-tramadol provides good quality of sedation and decreases perioperative analgesic requirements. To our knowledge, studies that use the combination of midazolam-tramadol for oral premedication in children undergoing adenotonsillectomy have not been widely reported in the literature.
The oral route of administration is the most popular choice in pediatric anesthesia for sedation, anxiolysis and anesthesia induction9. Various studies have indicated that oral midazolam fulfill many characteristics of the ideal pemedicant19. Cox et al. reviewed 30 scientific papers regarding the use of oral midazolam for premedication and concluded that it is effective in reducing both separation and induction anxiety in children, with minimal effect on recovery times2. In the current study, 86.6% of children in group M presented effective sedation (sedation score 2 or 3).
Tramadol is an effective opioid analgesic that binds with low affinity to m-opioid receptors20. The drug is most commonly used as an analgesic and less commonly as sedative agent. After oral administration in adults, tramadol capsules demonstrate a bioavailability of 68% due to an 18 to 30% first-pass metabolism, following absorption from the upper small intestine. The peak plasma level in adults is reached within 2h, with analgesia commencing at between 20 to 40 minutes21. In a pediatric oral tramadol drops study, absorption was unexpectedly rapid. The highest measured serum concentration was the first one at 30 minutes, suggesting that the peak level may have already taken place. If the pattern of the serum concentration of tramadol following oral administration closely follows the one after intravenous administration, it would be expected that it’s metabolite peak serum concentration would also be similar14.
There is no single drug available that meet all the requirements of an ideal drug. Drug combinations are therefore a useful alternative for premedication of pediatric surgical population. To overcome the drawbacks and disadvantages when midazolam or tramadol is used alone, combination of both drugs in different doses have been used in order to improve sedation, success rate in premedication, but the results had shown marked variations21,22. Koirala et al. administered tramadol (2 mg/kg) as a sedative in combination with midazolam and zolpidem separately21. They showed that tramadol was less effective compared to midazolam considering analgesia and sedation in anxious and uncooperative child patients. Bhatnagar et al. used tramadol (2 mg/kg) as a sedative agent22. Their results were significantly different from previous studies. Earlier studies and literature state tramadol as an analgesic with lesser sedative potential21. In their study tramadol produced level of sedation as equivalent to midazolam. The ease of treatment was also as good as midazolam. In the present study, significantly more patients in group midazolam-tramadol (MT) presented sedation score 2 (sleep, but arousable) compared to patients in group of midazolam (M). Only one patient in group MT showed poor separation score compared to three patients in group M, while only two patients in group MT presented poor mask cooperation compared to four patients in group M.
In the study of Roelofse et al. children, aged 4-7 years, undergoing dental extractions received either tramadol drops at 1.5 mg/Kg or placebo23. Both groups received oral midazolam 0.5 mg/Kg, 30 minutes prior to surgery. Postoperative rescue analgesia was administrated to 19.4% of tramadol group compared with 82.8% of the placebo group. This approach showed the value of using effective analgesic drugs, before sedation in order to minimize postoperative pain. The results of this study confirmed the Roelofse et al. study, as the consumption of rescue analgesics was lower in patients of midazolam-tramadol group compared to midazolam group23. Pharmacokinetic studies showed that postoperative analgesia lasts up to 9 hours following oral tramadol14. In another study, children received tramadol drops 3 mg/kg with oral midazolam at 0.5 mg/kg; control group received only oral midazolam 0.5 mg/kg24. The results of the earlier studies demonstrated the analgesic effects of tramadol, it’s lack of respiratory depression in pediatric patients and normal recovery times, when used in combination with a sedative. Therefore the combination of oral tramadol (1-3 mg/kg) with midazolam is useful for sedation and postoperative pain control for pediatric surgical patients. In the present study, the analgesic efficacy of tramadol led patients of group MT to experience less pain and consume significantly lower amount of remifentanil intraoperatively compared to group M. Also, it is known that in order to achieve a minimal incidence of adverse effects with oral administration of tramadol, treatment should be commenced at the lowest dose25. Therefore in this study the dosage of 1 mg.kg-1 oral tramadol was selected. Emesis during recovery occurred only in one child in group MT.
Negus et al.26 reported that the combination of oral midazolam and intravenous morphine, as premedication, can cause upper respiratory airway obstruction in children. Vickers et al. reported that tramadol has no clinically relevance to respiratory depression27. It is worth noting that no significant incidence of respiratory depression following combined use of midazolam and tramadol were observed.
A quite, pain-free recovery from anesthesia with rapid return of reflexes with no retching or vomiting is desirable following adenotonsillectomy28. In this study, both groups did not delay significantly the recovery of spontaneous respiration at the end of anesthesia.
The major limitation of this study was related to the small sample size. However, this study may provide the basis for future trials in children.
In conclusion, within the limits of the present study it can be stated that midazolam (0.5 mg/kg) is effective premedication drug in producing sedation for the pediatric surgical patients, following adenotonsillectomy. Adding tramadol (1mg/kg) has produced a sedation level equivalent to midazolam and also provided better perioperative pain control.
REFERENCES
- Kain ZN, Mayes LC, O’Connor TZ, et al. Preoperative anxiety in children: predictors and outcomes. Arch Pediatr Adolesc Med 1996;150:1238 – 45.
- Bozkurt Premedication of the pediatric patient – anesthesia for the uncooperative child. Curr Opin Anaesthesiol. 2007;20:211-5.
- Kayaalp L, Bozkurt P, Odabasi G, et al. Psychological effects of repeated general anesthesia in children. Paediatr Anaesth 2006;16:822-7.
- Kain Z, Mayes L, Wang S, et al. Parental presence during induction of anesthesia vs. sedative premedication: Which intervention is more effective? Anesthesiol 1999;89:1147-56.
- Messeri A, Caprilli S, Busoni P. Anesthesia induction in children: A psychological evaluation of the efficiency of parents’ presence. Pediatr Anesth 2004;14:551-6
- Kogan A, Katz J, Efrat R, Eidelman LA. Premedication with midazolam in young children: A comparison of four routes of administration. Paediatr Anaesth 2002;12:685-9.
- Rabie M.E. Combination of oral ketamine and modazolam versus modazolam alone as a premedication in children undergoing tonsillectomy. AJAIC 2005;8:58-64.
- Raiger LK, Naithani U, Bhatia S,et al. Seizures after intravenous tramadol given as premedication. Indian J Anaesth. 2012;56:55-7.
- Payne KA, Roelofse JA, Shipton EA. Pharmacokinetics of oral tramadol drops for postoperative pain relief in children aged 4 to 7 years–a pilot study. Anesth Prog. 2002;49:109-12.
- Bayrak F, Gunday I, Memis D, et al. A comparison of oral midazolam, oral tramadol, and intranasal sufentanil premedication in pediatric patients. J Opioid Manag 2007;3:74-8.
- Epstein RH, Mendel HG, Witkowski TA et al. The safety and efficacy of oral ransmucosal fentanyl citrate for preoperative sedation in young children. Anesth Analg 1996;83:1200–5.
- Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth 1995;7:89 –91.
- Hannallah RS, Broadman LS, Belman AB et al. Comparison of caudal and ilioinguinal nerve blocks for control of postorchidopexy pain in pediatric ambulatory surgery. Anesthesiol 1987; 66: 832-4.
- Parnis SJ, Foate JA, van der Walt JH, et al. Oral midazolam is an effective premedication for children having day-stay anesthesia. Anesth Int Care 1992;20:9-14.
- Mehlisch DR. The efficacy of combination analgesic therapy in relieving dental pain. J Am Dent Assoc. 2002;133:861-71.
- Koirala B, Pandey RK, Saksen AK, et al. A comparative evaluation of newer sedatives in conscious sedation. J Clin Pediatr Dent 2006;30:273-6.
- Bhatnagar S, Das UM, Bhatnagar G. Comparison of oral midazolam with oral tramadol, triclofos and zolpidem in the sedation of pediatric dental patients: an in vivo study. J Indian Soc Pedod Prev Dent. 2012;30:109-14.
- Roelofse JA, Payne KA. Oral tramadol: analgesic efficacy in children following multiple dental extractions. Eur J Anaesthesiol. 1999;16:441-7.
- Payne KA, Roelofse JA. Tramadol drops in children: analgesic efficacy, lack of respiratory effects, and normal recovery times. Anesth Prog. 1999 ;46:91-6.
- Budd K, Langford R. Tramadol revisited. Br J Anaesth. 1999;82:493-5.
- Negus BH, Street NE. Midazolam-opioid combination and postoperative upper airway obstruction in children. Anaesth Intensive Care. 1994;22:232-3.
- Duthie DJ. Remifentanil and tramadol. Br J Anaesth. 1998 ;81:51-7.
- Van den Berg AA, Montoya-Pelaez LF, Halliday EM, et al. Analgesia for adenotonsillectomy in children and young adults: a comparison of tramadol, pethdine and nalbuphine. Eur J Anaesthesiol 1999;16:186-94.
- Honarmand A, Safavi M, Kashefi P, et al. Comparison of effect of intravenous ketamine, peritonsillar infiltration of tramadol and their combination on pediatric posttonsillectomy pain: A double-blinded randomized placebo-controlled clinical trial. Res Pharm Sci. 2013;8:177-83.
- Feld LH, Negus JB, White PF. Oral midazolam preanesthetic medication in pediatric outpatients. Anesthesiol 1990;73:831–4.
- Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43:879–923.
- Shadnia S, Soltaninejad K, Heydari K,et al . Tramadol intoxication: A review of 114 cases. Hum Exp Toxicol 2008;27:201-5.
- Sansone RA, Sansone LA. Tramadol: Seizures, serotonin syndrome, and coadministered antidepressants. Psychiatry (Edgmont) 2009;6:17-21.
Author Disclosures:
Authors Vrigga M, Papagiannopoulou P, Ntritsou V, Isaakidis A, Chatziiokimidis Ch, Kostoglou Ch and Zachariadou Ch have no conflicts of interest or financial ties to disclose.
Corresponding author:
Vrigga Malamati
Department of Anesthesiology,
“G.Gennimatas” General Hospital,
Thessaloniki, Greece
Tel: 2310963274
E-mail:






